Breast Medical Oncology Division, Istituto Nazionale Tumori IRCCS "Fondazione G. Pascale", Naples, Italy.
Medical Oncology Unit & Phase 1 Research Unit, ASST Monza, Monza, Italy.
BMC Cancer. 2020 Mar 19;20(1):232. doi: 10.1186/s12885-020-6707-9.
NEPA is an oral fixed-dose combination of netupitant, a new highly selective neurokinin-1 receptor antagonist, and palonosetron. This study was conducted to evaluate whether the efficacy of NEPA against chemotherapy-induced nausea and vomiting (CINV) in cycle 1 would be maintained over subsequent chemotherapy cycles in breast cancer patients receiving adjuvant anthracycline plus cyclophosphamide (AC). The study also describes the relationship between efficacy on day 1 through 5 (overall period) and control of CINV on day 6 through 21 (very late period) in each cycle.
In this multicentre, phase II study, patients received both NEPA and dexamethasone (12 mg intravenously) just before chemotherapy. The primary efficacy endpoint was overall complete response (CR; no emesis and no rescue medication use) in cycle 1. Sustained efficacy was evaluated during the subsequent cycles by calculating the rate of CR in cycles 2-4 and by assessing the probability of sustained CR over multiple cycles. The impact of both overall CR and risk factors for CINV on the control of very late events (vomiting and moderate-to-severe nausea) were also examined.
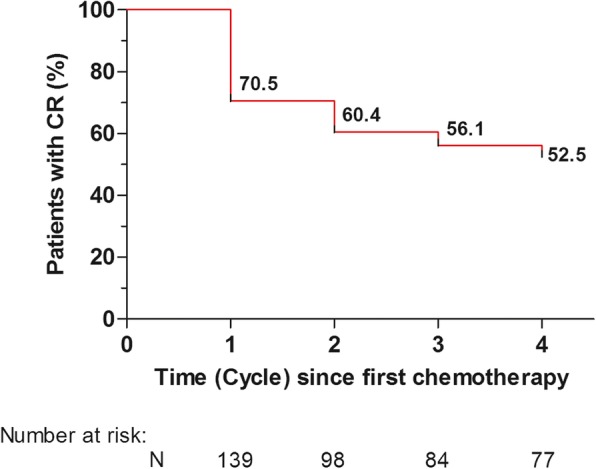
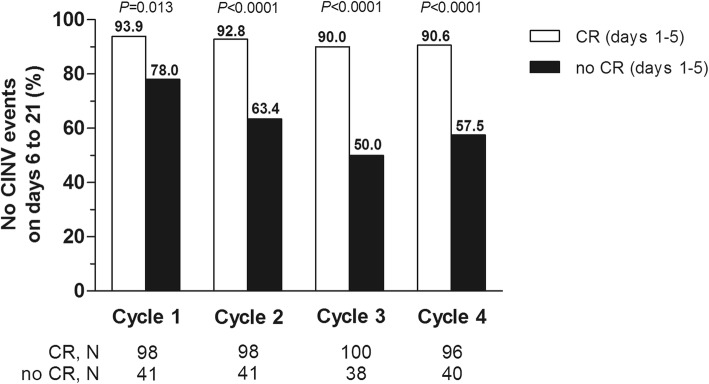
Of the 149 patients enrolled in the study, 139 were evaluable for a total of 552 cycles; 97.8% completed all 4 cycles. The proportion of patients with an overall CR was 70.5% (90% CI, 64.1 to 76.9) in cycle 1, and this was maintained in subsequent cycles. The cumulative percentage of patients with a sustained CR over 4 cycles was 53%. NEPA was well tolerated across cycles. In each cycle, patients with CR experienced a significantly better control of very late CINV events than those who experienced no CR. Among the patients with CR, the only predictor for increased likelihood of developing very late CINV was pre-chemotherapy (anticipatory) nausea (adjusted odds ratio = 0.65-0.50 for no CINV events on cycles 3 and 4).
The high anti-emetic efficacy seen with the NEPA regimen in the first cycle was maintained over multiple cycles of adjuvant AC for breast cancer. Preliminary evidence also suggests that patients achieving a CR during the overall period gain high protection even against very late CINV events in each chemotherapy cycle.
This trial was retrospectively registered at Clinicaltrials.gov identifier (NCT03862144) on 05/Mar/2019.
NEPA 是一种新型高选择性神经激肽-1 受体拮抗剂奈妥匹坦与帕洛诺司琼的口服固定剂量复方制剂。这项研究旨在评估 NEPA 在接受辅助蒽环类药物加环磷酰胺(AC)治疗的乳腺癌患者中,在第 1 周期中对化疗引起的恶心和呕吐(CINV)的疗效是否能在后续化疗周期中维持。该研究还描述了每个周期中第 1 至 5 天(总期)的疗效与第 6 至 21 天(迟发性期)的 CINV 控制之间的关系。
在这项多中心、二期研究中,患者在化疗前接受 NEPA 和地塞米松(12mg 静脉注射)。主要疗效终点是第 1 周期的总体完全缓解(CR;无呕吐且无解救药物使用)。通过计算第 2-4 周期的 CR 率,并评估多个周期的持续 CR 概率,来评估后续周期中的持续疗效。还检查了总体 CR 以及 CINV 风险因素对迟发性事件(呕吐和中重度恶心)控制的影响。
在纳入研究的 149 名患者中,共有 139 名患者在总共 552 个周期中可进行评估;97.8%的患者完成了所有 4 个周期。第 1 周期的患者总体 CR 比例为 70.5%(90%可信区间,64.1 至 76.9),且在后续周期中得以维持。4 个周期内持续 CR 的患者累计百分比为 53%。NEPA 在各周期中均耐受良好。在每个周期中,CR 的患者与无 CR 的患者相比,迟发性 CINV 事件的控制情况明显更好。在 CR 的患者中,唯一增加迟发性 CINV 风险的预测因素是化疗前(预期性)恶心(无第 3 和第 4 周期 CINV 事件的调整优势比为 0.65-0.50)。
NEPA 方案在第一周期的高止吐疗效在辅助 AC 治疗乳腺癌的多个周期中得以维持。初步证据还表明,在总期间达到 CR 的患者即使在每个化疗周期中也能获得对迟发性 CINV 事件的高度保护。
该试验于 2019 年 3 月 5 日在 Clinicaltrials.gov 登记(NCT03862144)。