Department of Cardiology, Odense University Hospital, J. B. Winsløwsvej 4, Odense C, Denmark.
Department of Cardiology, Rigshospitalet, Copenhagen University Hospital, Copenhagen, Denmark.
Crit Care. 2020 Mar 18;24(1):95. doi: 10.1186/s13054-020-2816-8.
Concomitant vasoactive drugs are often required to maintain adequate perfusion pressure in patients with acute myocardial infarction (AMI) and cardiogenic shock (CS) receiving hemodynamic support with an axial flow pump (Impella CP).
To compare the effect of equipotent dosages of epinephrine, dopamine, norepinephrine, and phenylephrine on cardiac work and end-organ perfusion in a porcine model of profound ischemic CS supported with an Impella CP.
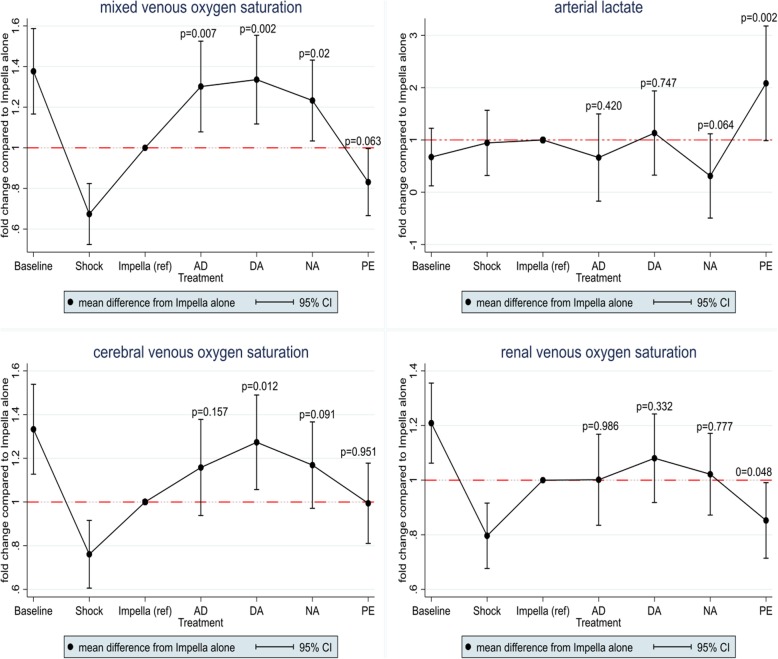
CS was induced in 10 pigs by stepwise intracoronary injection of polyvinyl microspheres. Hemodynamic support with Impella CP was initiated followed by blinded crossover to vasoactive treatment with norepinephrine (0.10 μg/kg/min), epinephrine (0.10 μg/kg/min), or dopamine (10 μg/kg/min) for 30 min each. At the end of the study, phenylephrine (10 μg/kg/min) was administered for 20 min. The primary outcome was cardiac workload, a product of pressure-volume area (PVA) and heart rate (HR), measured using the conductance catheter technique. End-organ perfusion was assessed by measuring venous oxygen saturation from the pulmonary artery (SvO), jugular bulb, and renal vein. Treatment effects were evaluated using multilevel mixed-effects linear regression.
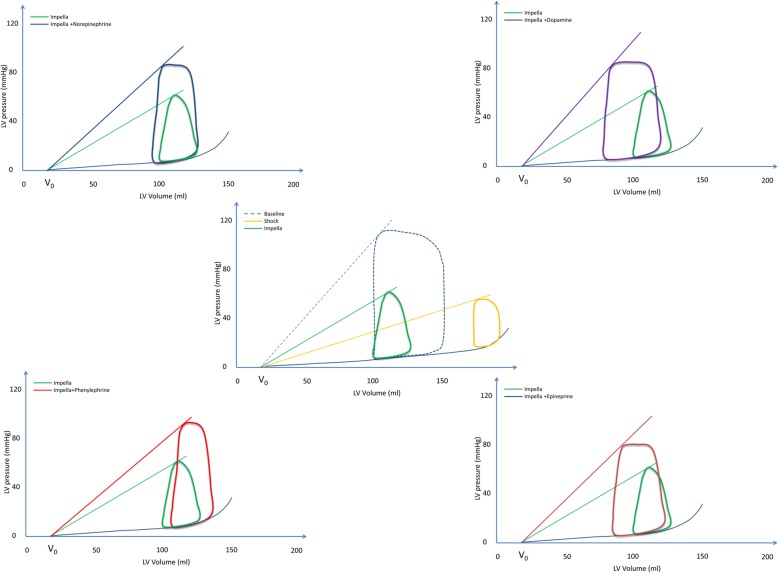
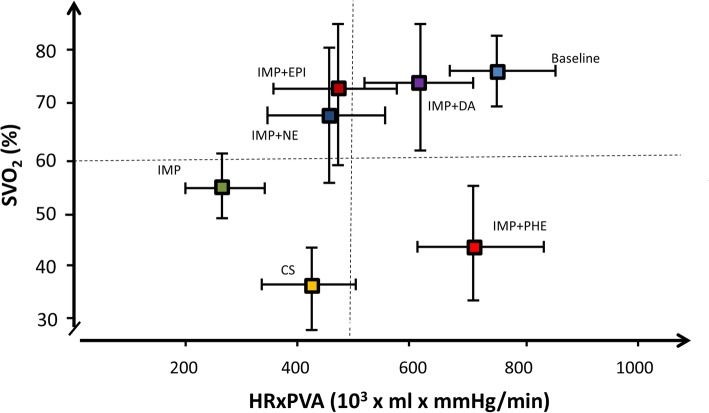
All catecholamines significantly increased LV stroke work and cardiac work, dopamine to the greatest extend by 341.8 × 10 (mmHg × mL)/min [95% CI (174.1, 509.5), p < 0.0001], and SvO significantly improved during all catecholamines. Phenylephrine, a vasoconstrictor, caused a significant increase in cardiac work by 437.8 × 10 (mmHg × mL)/min [95% CI (297.9, 577.6), p < 0.0001] due to increase in potential energy (p = 0.001), but no significant change in LV stroke work. Also, phenylephrine tended to decrease SvO (p = 0.063) and increased arterial lactate levels (p = 0.002).
Catecholamines increased end-organ perfusion at the expense of increased cardiac work, most by dopamine. However, phenylephrine increased cardiac work with no increase in end-organ perfusion.
在接受轴向血流泵(Impella CP)血流动力学支持的急性心肌梗死(AMI)和心源性休克(CS)患者中,常需要同时使用血管活性药物来维持足够的灌注压。
比较等剂量的肾上腺素、多巴胺、去甲肾上腺素和苯肾上腺素对使用 Impella CP 支持的严重缺血性 CS 猪模型中心脏做功和终末器官灌注的影响。
通过逐步冠状动脉内注射聚氯乙烯微球诱导 10 头猪发生 CS。启动 Impella CP 血流动力学支持,然后进行盲法交叉至血管活性药物治疗,分别用去甲肾上腺素(0.10μg/kg/min)、肾上腺素(0.10μg/kg/min)或多巴胺(10μg/kg/min)治疗 30min。研究结束时,给予苯肾上腺素(10μg/kg/min)治疗 20min。主要结局指标是使用电导导管技术测量的压力-容积面积(PVA)和心率(HR)乘积的心脏工作量。终末器官灌注通过测量肺动脉(SvO)、颈静脉球和肾静脉的静脉血氧饱和度来评估。使用多级混合效应线性回归评估治疗效果。
所有儿茶酚胺均显著增加 LV 射血做功和心脏做功,多巴胺增加最多,为 341.8×10(mmHg×mL)/min[95%置信区间(174.1,509.5),p<0.0001],SvO 在所有儿茶酚胺治疗期间均显著改善。血管收缩剂苯肾上腺素通过增加势能使心脏做功显著增加 437.8×10(mmHg×mL)/min[95%置信区间(297.9,577.6),p<0.0001],但 LV 射血做功无显著变化。此外,苯肾上腺素倾向于降低 SvO(p=0.063)并增加动脉乳酸水平(p=0.002)。
儿茶酚胺以增加心脏做功为代价增加终末器官灌注,其中以多巴胺增加最多。然而,苯肾上腺素增加了心脏做功,而终末器官灌注没有增加。