Department of Pathology, Ewha Womans University Seoul Hospital, Ewha Womans University College of Medicine, Seoul, Korea.
Department of Radiology, Research Institute of Radiological Science, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
PLoS One. 2020 Mar 20;15(3):e0230622. doi: 10.1371/journal.pone.0230622. eCollection 2020.
Circulating tumor DNA (ctDNA) is cell-free DNA that is released into peripheral blood by tumor cells. ctDNA harbors somatic mutations and mutant ctDNA obtained from blood can be used as a biomarker in advanced non-small cell lung cancer (NSCLC). In this study, we investigated the clinicopathological properties of tumors that shed ctDNA in surgically resected NSCLC patients.
Consecutive cases of NSCLC with matching surgically resected tissue specimens and peripheral or specimen blood samples were eligible for this study. EGFR and KRAS mutations in plasma ctDNA and formalin-fixed paraffin-embedded tissue were analyzed using peptide nucleic acid clamping-assisted method. The plasma and tissue results were compared according to clinicopathological features.
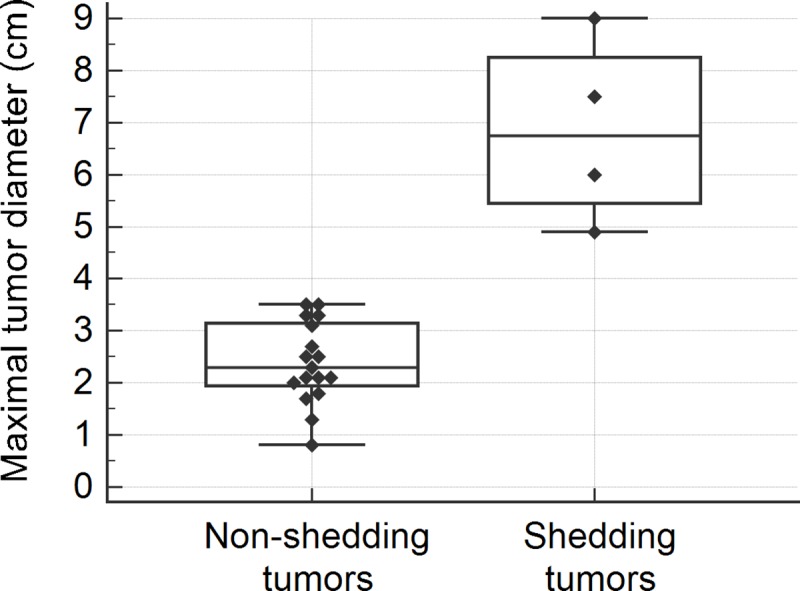
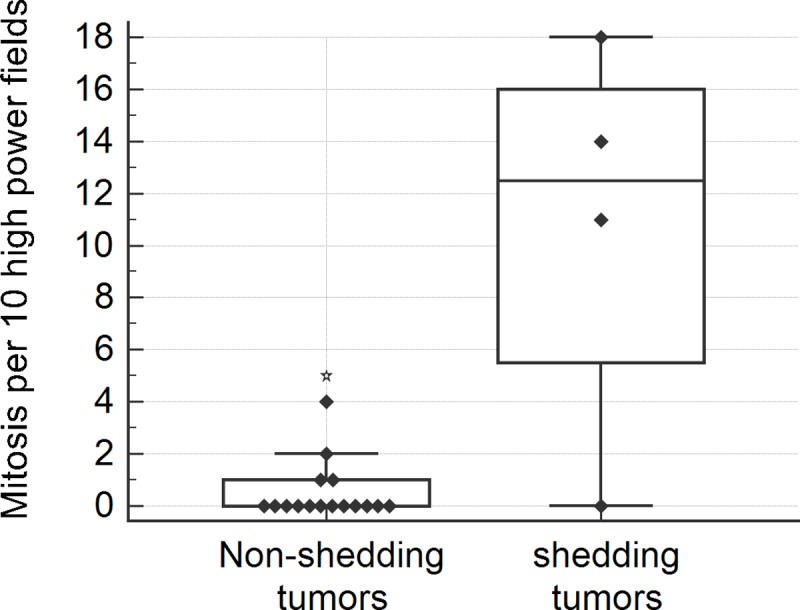
Mutation analyses were available for 36 cases. EGFR and KRAS mutations were present in 41.7% (15/36) and 16.7% (6/36) of tissue samples, respectively. Among EGFR and KRAS-mutant tumors, plasma mutation detection sensitivity was 13.3% (2/15) for EGFR and 33.3% (2/6) for KRAS. The presence of ctDNA in plasma was significantly associated with higher pathological tumor stage (p = 0.028), nodal metastasis (p = 0.016), solid adenocarcinoma pattern (p = 0.003), tumor necrosis (p = 0.012), larger primary tumor diameter (p = 0.002) or volume (p = 0.002), and frequent mitosis (p = 0.018) in tissue specimens. All tumors larger than 4 cm in maximal diameter or 25 cm3 in volume shed ctDNA in plasma. In subgroup analysis among EGFR mutated adenocarcinoma, ctDNA was significantly associated with nodal metastasis (p = 0.029), vascular invasion (p = 0.029), solid adenocarcinoma pattern (p = 0.010), and tumor necrosis (p = 0.010), high mitotic rate (p = 0.009), large pathological tumor size (p = 0.027), and large tumor volume on CT (p = 0.027).
We suggest that primary or total tumor burden, solid adenocarcinoma morphology, tumor necrosis, and frequent mitosis could predict ctDNA shedding in pulmonary adenocarcinoma.
循环肿瘤 DNA(ctDNA)是由肿瘤细胞释放到外周血中的无细胞 DNA。ctDNA 携带体细胞突变,从血液中获得的突变 ctDNA 可用作晚期非小细胞肺癌(NSCLC)的生物标志物。在这项研究中,我们研究了手术切除 NSCLC 患者中释放 ctDNA 的肿瘤的临床病理特征。
连续入选有匹配手术切除组织标本和外周血或标本血样的 NSCLC 病例符合本研究标准。采用肽核酸夹辅助法分析血浆 ctDNA 和福尔马林固定石蜡包埋组织中的 EGFR 和 KRAS 突变。根据临床病理特征比较血浆和组织结果。
36 例可进行突变分析。组织样本中分别有 41.7%(15/36)和 16.7%(6/36)存在 EGFR 和 KRAS 突变。在 EGFR 和 KRAS 突变肿瘤中,血浆突变检测的敏感性为 EGFR 为 13.3%(2/15),KRAS 为 33.3%(2/6)。血浆中存在 ctDNA 与较高的病理肿瘤分期(p=0.028)、淋巴结转移(p=0.016)、实性腺癌形态(p=0.003)、肿瘤坏死(p=0.012)、原发肿瘤直径较大(p=0.002)或体积较大(p=0.002)、组织标本中频繁有丝分裂(p=0.018)显著相关。所有最大直径大于 4 cm 或体积大于 25 cm3 的肿瘤均在血浆中释放 ctDNA。在 EGFR 突变的腺癌亚组分析中,ctDNA 与淋巴结转移(p=0.029)、血管侵犯(p=0.029)、实性腺癌形态(p=0.010)、肿瘤坏死(p=0.010)、高有丝分裂率(p=0.009)、较大的病理肿瘤大小(p=0.027)和 CT 上较大的肿瘤体积(p=0.027)显著相关。
我们认为原发或总肿瘤负荷、实性腺癌形态、肿瘤坏死和频繁有丝分裂可预测肺腺癌中 ctDNA 的释放。