Hunderi Jon Olav Gjengstø, Rolfsjord Leif Bjarte, Carlsen Karin C Lødrup, Holst René, Bakkeheim Egil, Berents Teresa Løvold, Carlsen Kai-Håkon, Skjerven Håvard Ove
Dept of Pediatrics and Adolescent Medicine, Østfold Hospital Trust, Grålum, Norway.
Division of Pediatric and Adolescent Medicine, Oslo University Hospital, Oslo, Norway.
ERJ Open Res. 2020 Mar 16;6(1). doi: 10.1183/23120541.00268-2019. eCollection 2020 Jan.
Acute bronchiolitis during infancy and human rhinovirus (HRV) lower respiratory tract infections increases the risk of asthma in atopic children. We aimed to explore whether specific viruses, allergic sensitisation or cortisol levels during acute bronchiolitis in infancy increase the risk of early asthma, using recurrent wheeze as a proxy.
In 294 children with a mean (range) age of 4.2 (0-12) months enrolled during hospitalisation for acute infant bronchiolitis, we analysed virus in nasopharyngeal aspirates, serum specific immunoglobulin E against food and inhalant allergens, and salivary morning cortisol. These factors were assessed by regression analyses, adjusted for age, sex and parental atopy, for risk of recurrent wheeze, defined as a minimum of three parentally reported episodes of wheeze at the 2-year follow-up investigation.
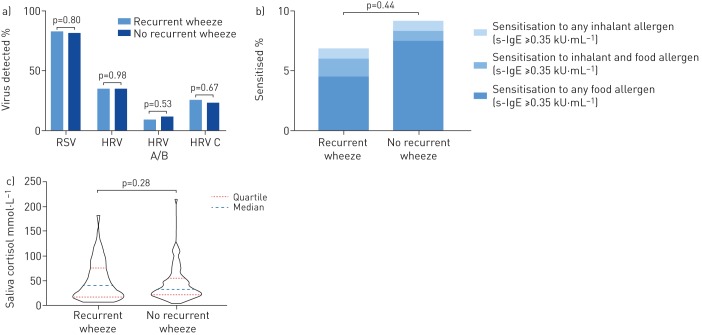
At 2 years, children with, compared to without, recurrent wheeze had similar rates of respiratory syncytial virus (RSV) (82.9% 81.8%) and HRV (34.9% 35.0%) at the acute bronchiolitis, respectively. During infancy, 6.9% of children with and 9.2% of children without recurrent wheeze at 2 years were sensitised to at least one allergen (p=0.5). Neither recurrent wheeze nor incidence rate ratios for the number of wheeze episodes at 2 years were significantly associated with specific viruses, high viral load of RSV or HRV, allergic sensitisation, or morning salivary cortisol level during acute bronchiolitis in infancy.
In children hospitalised with acute infant bronchiolitis, specific viruses, viral load, allergic sensitisation and salivary morning cortisol did not increase the risk of early asthma by 2 years of age.
婴儿期急性细支气管炎和人鼻病毒(HRV)引起的下呼吸道感染会增加特应性儿童患哮喘的风险。我们旨在探讨婴儿期急性细支气管炎期间的特定病毒、过敏致敏或皮质醇水平是否会增加早期哮喘的风险,以反复喘息作为替代指标。
在294名因急性婴儿细支气管炎住院的平均(范围)年龄为4.2(0 - 12)个月的儿童中,我们分析了鼻咽抽吸物中的病毒、针对食物和吸入性过敏原的血清特异性免疫球蛋白E以及唾液早晨皮质醇。通过回归分析评估这些因素,并对年龄、性别和父母特应性进行校正,以评估反复喘息的风险,反复喘息定义为在2年随访调查中至少有三次家长报告的喘息发作。
在2岁时,与无反复喘息的儿童相比,有反复喘息的儿童在急性细支气管炎时呼吸道合胞病毒(RSV)(82.9%对81.8%)和HRV(34.9%对35.0%)的感染率相似。在婴儿期,2岁时有反复喘息的儿童中有6.9%、无反复喘息的儿童中有9.2%对至少一种过敏原致敏(p = 0.5)。婴儿期急性细支气管炎期间的反复喘息或2岁时喘息发作次数的发病率比值均与特定病毒、RSV或HRV的高病毒载量、过敏致敏或早晨唾液皮质醇水平无显著关联。
在因急性婴儿细支气管炎住院的儿童中,特定病毒、病毒载量、过敏致敏和唾液早晨皮质醇不会增加2岁时早期哮喘的风险。