Zumsteg Daniel M, Chu Caleb Everett, Midwinter Mark John
School of Biomedical Sciences, University of Queensland Faculty of Medicine and Biomedical Sciences, Brisbane, Queensland, Australia.
Jamieson Trauma Institute, MetroNorth Hopsital and Health Service, Brisbane, Queensland, Australia.
Trauma Surg Acute Care Open. 2020 Mar 15;5(1):e000414. doi: 10.1136/tsaco-2019-000414. eCollection 2020.
Compared with similarly injured patients of a younger age, elderly patients have worse outcomes from acute injury. One factor adversely affecting outcomes is sarcopenia, which has been assessed in healthy elderly populations through established clinical and radiological criteria. However, in the acute care setting, no such criteria have been established. Sarcopenia has been opportunistically assessed via radiographic means but there is as of yet no gold standard. The purpose of this review is to summarize the radiological methods used to diagnose sarcopenia in the acute care setting, and suggest ways in which these methods may lead to a consensus definition of sarcopenia and its relationship to patient outcomes.
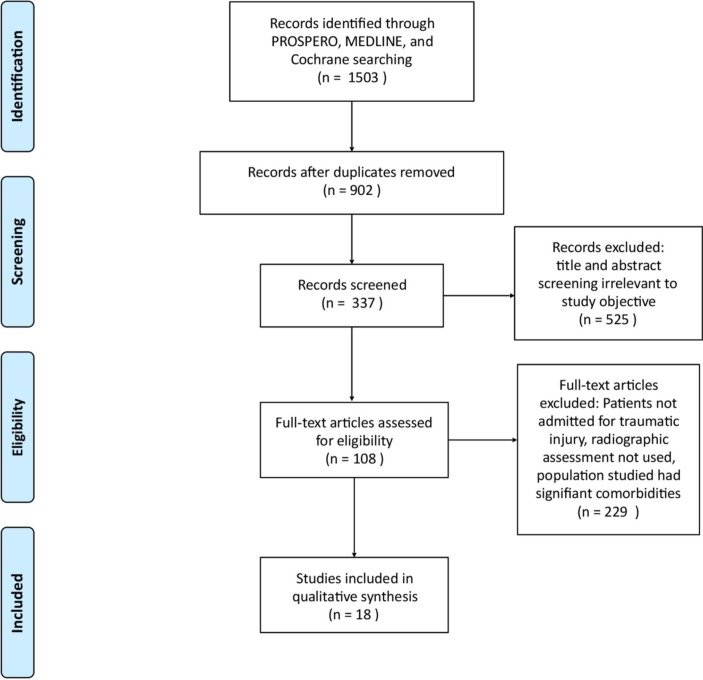
A systematic survey of medical databases was conducted, with 902 unique publications identified. After screening and application of inclusion and exclusion criteria, data regarding study population, outcome, imaging modality, and criteria for assessment of sarcopenia were extracted from 20 studies. Quality was assessed with the Newcastle-Ottawa Scale.
CT was the imaging modality for 18 of the studies, with total psoas muscle cross-sectional area at the level of L3 and L4 being the dominant method for assessing sarcopenia. Adjustment for body morphology most commonly used patient height or L4 vertebral body area. The majority of articles found radiographically assessed sarcopenia to be significantly correlated to outcomes such as mortality, length of hospital stay, morbidity, and in-hospital complications.
Establishing a consistent definition would strengthen its applicability and generalizability to admission and discharge planning.
Systematic review, level III.
与年龄较轻的类似受伤患者相比,老年患者急性损伤的预后较差。影响预后的一个不利因素是肌肉减少症,已通过既定的临床和放射学标准在健康老年人群中进行了评估。然而,在急性护理环境中,尚未建立此类标准。肌肉减少症已通过影像学方法进行了机会性评估,但尚无金标准。本综述的目的是总结在急性护理环境中用于诊断肌肉减少症的放射学方法,并提出这些方法可能导致肌肉减少症的共识定义及其与患者预后关系的方式。
对医学数据库进行了系统调查,共识别出902篇独特的出版物。在筛选并应用纳入和排除标准后,从20项研究中提取了有关研究人群、结局、成像方式和肌肉减少症评估标准的数据。采用纽卡斯尔-渥太华量表评估质量。
18项研究的成像方式为CT,以L3和L4水平的腰大肌总横截面积作为评估肌肉减少症的主要方法。身体形态调整最常用的是患者身高或L4椎体面积。大多数文章发现,影像学评估的肌肉减少症与死亡率、住院时间、发病率和住院并发症等结局显著相关。
建立一致的定义将加强其在入院和出院计划中的适用性和普遍性。
系统评价,III级。