Department of Cardiovascular Medicine Sydell and Arnold Miller Family Heart & Vascular Institute Cleveland Clinic Foundation Cleveland OH.
Department of Thoracic and Cardiovascular Surgery Sydell and Arnold Miller Family Heart & Vascular Institute Cleveland Clinic Foundation Cleveland OH.
J Am Heart Assoc. 2020 Apr 7;9(7):e014591. doi: 10.1161/JAHA.119.014591. Epub 2020 Mar 24.
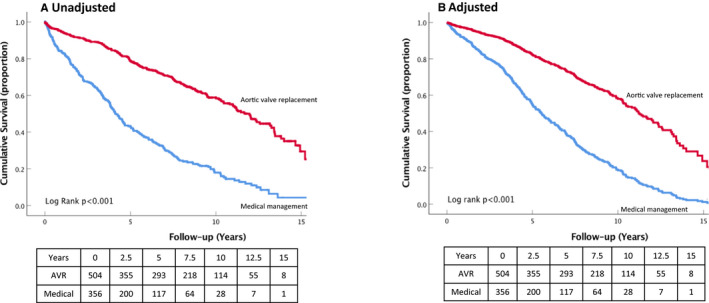
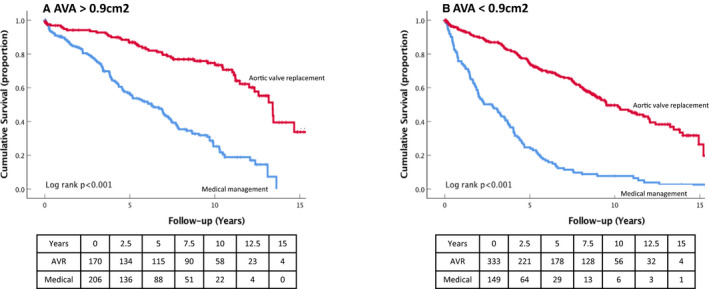
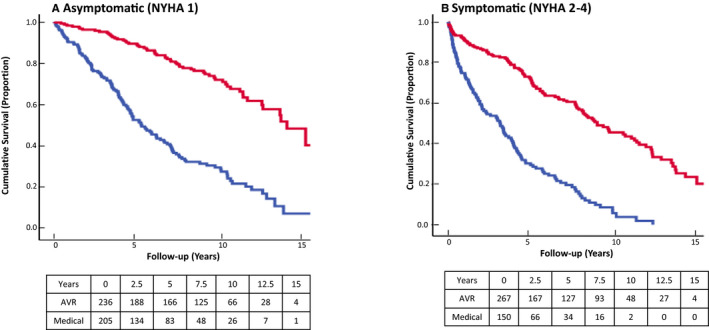
Background Concurrent presence of aortic stenosis and aortic regurgitation is termed mixed aortic valve disease (MAVD). Although multiple articles have addressed patients with "isolated" aortic stenosis or aortic regurgitation, the natural history, impact, and outcomes of MAVD are not well defined. Here, we evaluate long-term outcomes in patients with MAVD and cardiovascular adaptations to chronic MAVD. Methods and Results This observational cohort study evaluated 862 adult patients (56.8% male) with preserved left ventricular ejection fraction and at least moderate aortic regurgitation and moderate aortic stenosis. Primary outcome was all-cause mortality. Subgroup analysis was based on treatment modality (aortic valve replacement [AVR] versus medical management). A regression analysis of longitudinal echocardiographic parameters was performed to assess the natural history of MAVD. Mean age was 68±15 years, and mean left ventricular ejection fraction was 58±5%. At 4.6 years (25th-75th percentile range, 1.0-8.7), 58.6% of patients underwent an AVR and 48.8% patients died. In both unadjusted and adjusted Cox survival analysis, AVR was associated with improved survival (hazard ratio, 0.41; 95% CI, 0.34-0.51, <0.001). Impact of AVR persisted when stratifying the cohort by symptom status and baseline aortic valve area (log rank, <0.001 for both) and after propensity-score matching (hazard ratio, 0.40; 95% CI, 0.32-0.50; <0.001). In the longitudinal analysis, there were statistically significant changes over time in aortic valve peak gradient (<0.001) and aortic valve area (<0.001) and only mild increases in left ventricular end-diastolic (<0.007) and -systolic (<0.001) volumes. Conclusions MAVD confers a high risk of all-cause mortality. However, AVR significantly reduces this risk independent of aortic valve area, symptom status, and after controlling for confounding variables.
主动脉瓣狭窄和主动脉瓣反流同时存在称为混合性主动脉瓣疾病(MAVD)。虽然有许多文章讨论了“孤立性”主动脉瓣狭窄或主动脉瓣反流患者,但 MAVD 的自然史、影响和结局尚不清楚。在这里,我们评估了 MAVD 患者的长期结局以及慢性 MAVD 对心血管的适应性。
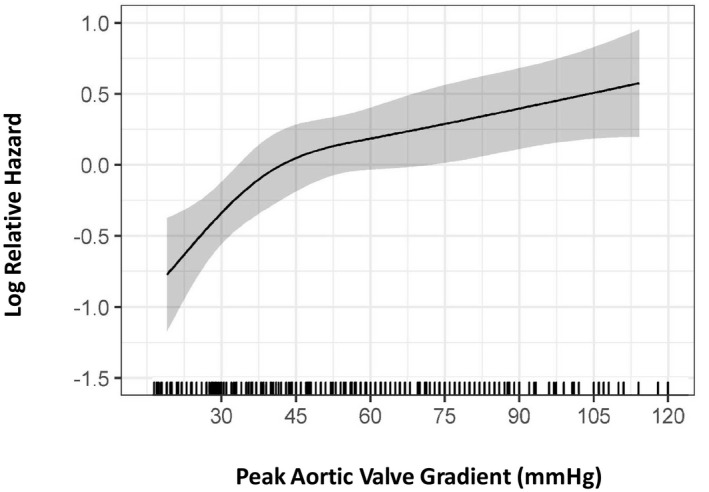
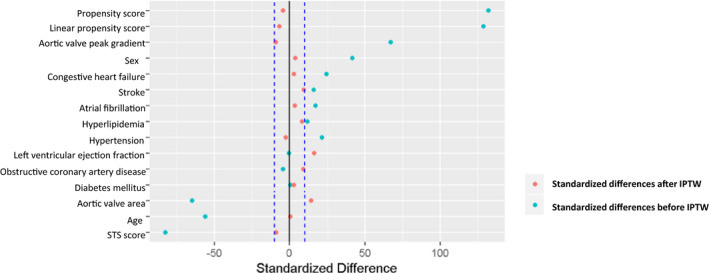
本观察性队列研究评估了 862 名左心室射血分数保留且至少有中度主动脉瓣反流和中度主动脉瓣狭窄的成年患者(56.8%为男性)。主要结局为全因死亡率。根据治疗方式(主动脉瓣置换[AVR]与药物治疗)进行亚组分析。对纵向超声心动图参数进行回归分析,以评估 MAVD 的自然史。平均年龄为 68±15 岁,平均左心室射血分数为 58±5%。在 4.6 年(25%至 75%范围,1.0-8.7)时,58.6%的患者接受了 AVR,48.8%的患者死亡。在未调整和调整后的 Cox 生存分析中,AVR 与生存率提高相关(风险比,0.41;95%CI,0.34-0.51,<0.001)。在按症状状态和基线主动脉瓣面积分层的队列中(对数秩检验,均<0.001)以及在倾向评分匹配后(风险比,0.40;95%CI,0.32-0.50;<0.001),AVR 的影响仍然存在。在纵向分析中,主动脉瓣峰值梯度(<0.001)和主动脉瓣面积(<0.001)随时间有统计学意义的变化,左心室舒张末期(<0.007)和收缩末期(<0.001)容积仅略有增加。
MAVD 导致全因死亡率高。然而,AVR 可显著降低这种风险,与主动脉瓣面积、症状状态以及控制混杂变量无关。