Grieve Stacy, Ding Keyue, Moore Jonathan, Finniss Mathew, Ray Ayush, Lees Miranda, Hossain Faisal, Murugesan Alli, Agar Jane, Acar Cenk, Taylor James, Shepherd Frances A, Reiman Tony
Department of Biology, University of New Brunswick Saint John, Saint John, New Brunswick, Canada.
Canadian Cancer Trials Group, Kingston, Ontario, Canada.
ESMO Open. 2020 Mar;5(2). doi: 10.1136/esmoopen-2020-000679.
There are no validated approaches to predict benefit from adjuvant chemotherapy for resected patients with non-small-cell lung cancer (NSCLC). The aim of this study was to translate a 15-gene mRNA expression profile published by Zhu shown to be prognostic and predictive of benefit, into a readily applicable immunohistochemistry (IHC) panel.
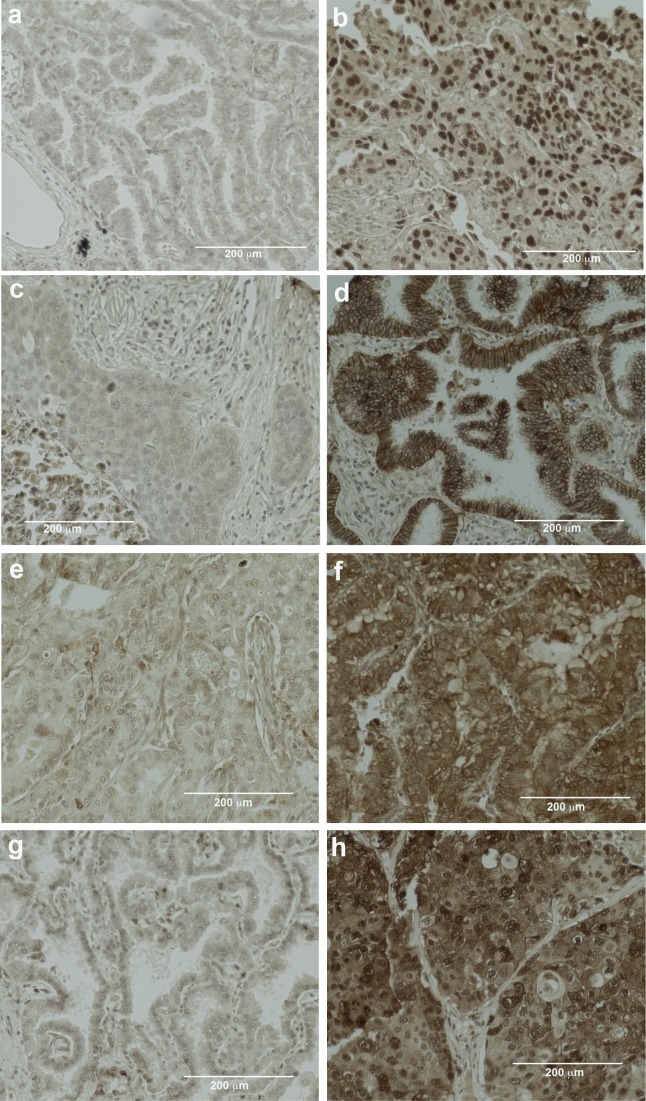
For seven of the genes in the gene expression profile (GEP) for which suitable commercial antibodies were available, we semiquantitatively assessed the IHC expression and prognostic significance for 173 patients treated at the Saint John Regional Hospital (SJRH). Cut-offs for high and low expression were defined for each marker and applied to IHC scores from 291 of the 482 patients in JBR.10, including patients on both the adjuvant chemotherapy and observation arms. The prognostic and predictive value of these markers on overall survival (OS) or recurrence-free survival (RFS) was assessed by Cox regression models.
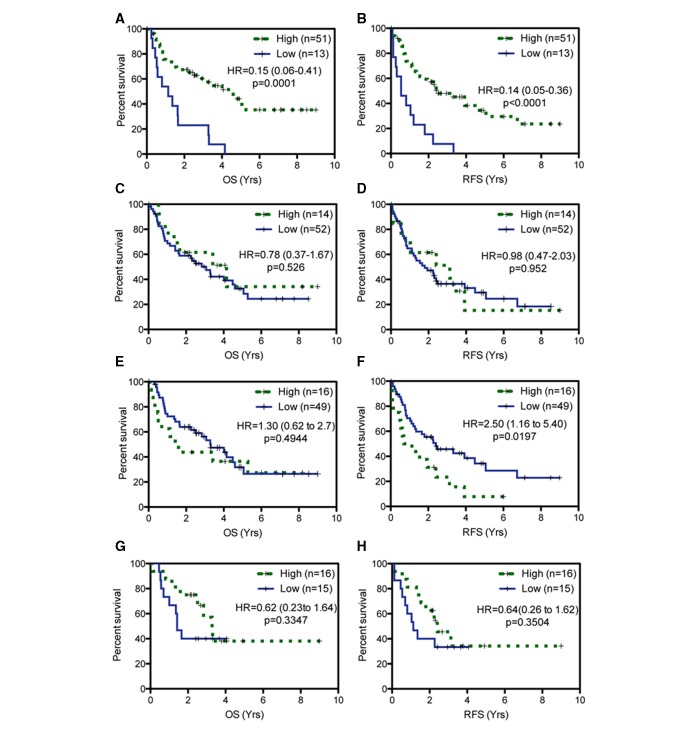
In the SJRH cohort, in 62 patients with resected stage II-III NSCLC, the prognostic significance of IHC assays for four proteins were concordant with Zhu's GEP results. Low FOSL2 (OS, HR=0.15; p=0.0001; RFS, HR=0.14; p<0.0001) and high STMN2 (RFS, HR=2.501; p=0.0197) were adverse prognostic factors. Low ATP1B1 and low TRIM14 expression trended toward worse OS and RFS. Validation of these markers with JBR.10 patients failed to show prognostic significance either individually or in combined risk classifications. Additionally, the interaction between these markers and chemotherapy treatment in predicting OS (FOSL2, p=0.52; STMN2 p=0.14; ATP1B1, p=0.33; TRIM14, p=0.81) or RFS (FOSL2, p=0.63; STMN2, p=0.12; ATP1B1, p=0.66; TRIM14, p=0.57) did not reach significance, individually or in combination panels.
Zhu's GEP could not be translated into an IHC panel predictive of benefit from adjuvant chemotherapy. Future predictive biomarker analysis in the adjuvant NSCLC setting may need to focus on novel therapies.
对于接受手术切除的非小细胞肺癌(NSCLC)患者,目前尚无经过验证的方法来预测辅助化疗的获益情况。本研究的目的是将Zhu发表的一个显示具有预后及预测获益价值的15基因mRNA表达谱,转化为一种易于应用的免疫组化(IHC)检测方法。
对于基因表达谱(GEP)中的7个基因,若有合适的商用抗体,我们对圣约翰地区医院(SJRH)接受治疗的173例患者的IHC表达及预后意义进行了半定量评估。为每个标志物定义了高表达和低表达的临界值,并将其应用于JBR.10研究中482例患者中的291例患者的IHC评分,包括辅助化疗组和观察组的患者。通过Cox回归模型评估这些标志物对总生存期(OS)或无复发生存期(RFS)的预后及预测价值。
在SJRH队列中,62例接受手术切除的II - III期NSCLC患者中,4种蛋白的IHC检测的预后意义与Zhu的GEP结果一致。FOSL2低表达(OS,HR = 0.15;p = 0.0001;RFS,HR = 0.14;p < 0.0001)和STMN2高表达(RFS,HR = 2.501;p = 0.0197)是不良预后因素。ATP1B1低表达和TRIM14低表达有OS和RFS变差的趋势。对JBR.10研究中的患者验证这些标志物,无论是单个标志物还是联合风险分类,均未显示出预后意义。此外,这些标志物与化疗治疗在预测OS(FOSL2,p = 0.52;STMN2,p = 0.14;ATP1B1,p = 0.33;TRIM14,p = 0.81)或RFS(FOSL2,p = 0.63;STMN2,p = 0.12;ATP1B1,p = 0.66;TRIM14,p = 0.57)方面的相互作用,无论是单个还是联合检测,均未达到显著水平。
Zhu的GEP无法转化为可预测辅助化疗获益的IHC检测方法。未来在辅助NSCLC治疗中进行预测性生物标志物分析可能需要关注新型疗法。