Department of Clinical Epidemiology and Medical Technology Assessment (KEMTA), Maastricht University Medical Centre+, The Netherlands.
Care and Public Health Research Institute (CAPHRI), Maastricht University, The Netherlands.
Eur J Prev Cardiol. 2020 Sep;27(13):1354-1365. doi: 10.1177/2047487320913380. Epub 2020 Mar 29.
Dual pathway inhibition with 2.5 mg rivaroxaban twice daily plus 100 mg aspirin once daily may be a promising alternative to 100 mg aspirin antiplatelet therapy for the prevention of cardiovascular events in patients with coronary artery disease and/or peripheral arterial disease. However, treatment costs and bleeding risks are higher, and there is another treatment option for peripheral arterial disease, 75 mg clopidogrel. A comprehensive assessment of benefits, risks and costs of dual pathway inhibition versus standard of care is needed.
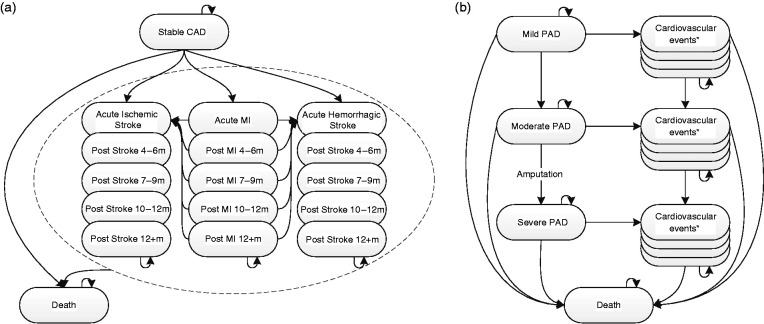
We used a state transition model including cardiovascular, ischaemic limb and bleeding events to compare dual pathway inhibition to aspirin antiplatelet therapy in coronary artery disease, and additionally to clopidogrel antiplatelet therapy in peripheral arterial disease patients. We calculated the incremental cost-effectiveness ratio from costs and quality-adjusted life-years of lifelong treatment, and the cost-effectiveness probability at a €50,000/quality-adjusted life-year threshold.
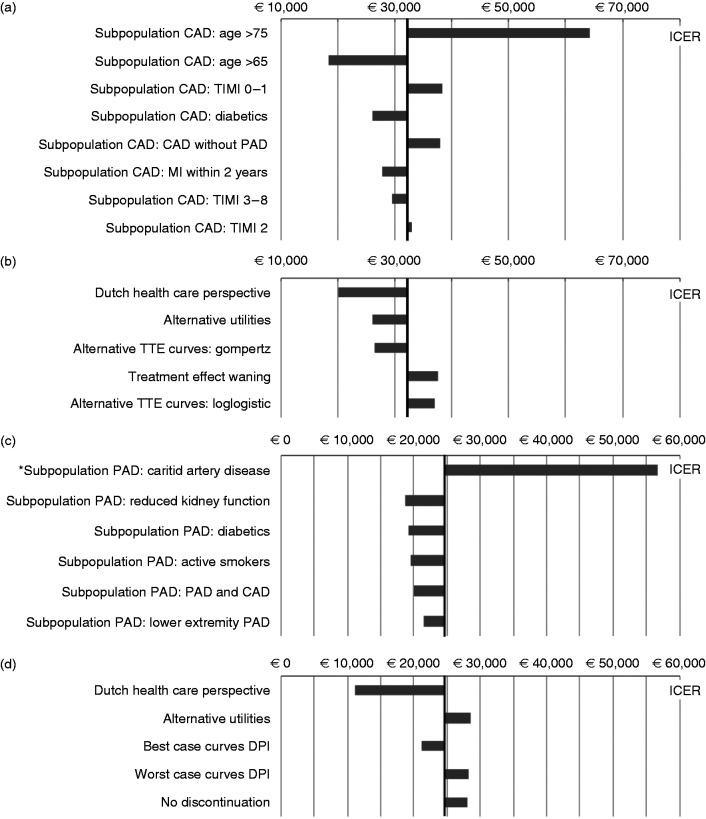
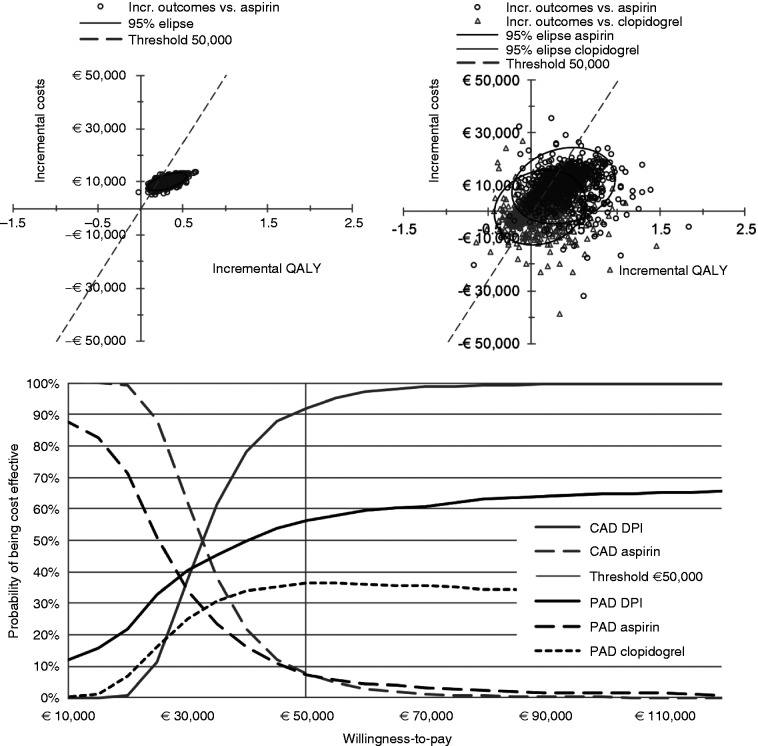
Quality-adjusted life-years and costs of dual pathway inhibition were highest, the incremental cost-effectiveness ratios versus aspirin were €32,109 in coronary artery disease and €26,381 in peripheral arterial disease patients, with 92% and 56% cost-effectiveness probability, respectively (clopidogrel was extendedly dominated). Incremental cost-effectiveness ratios were below €20,000 in comorbid peripheral arterial disease patients and coronary artery disease patients younger than 65 years, incremental cost-effectiveness ratios were above €50,000 in carotid artery disease patients and coronary artery disease patients older than 75 years.
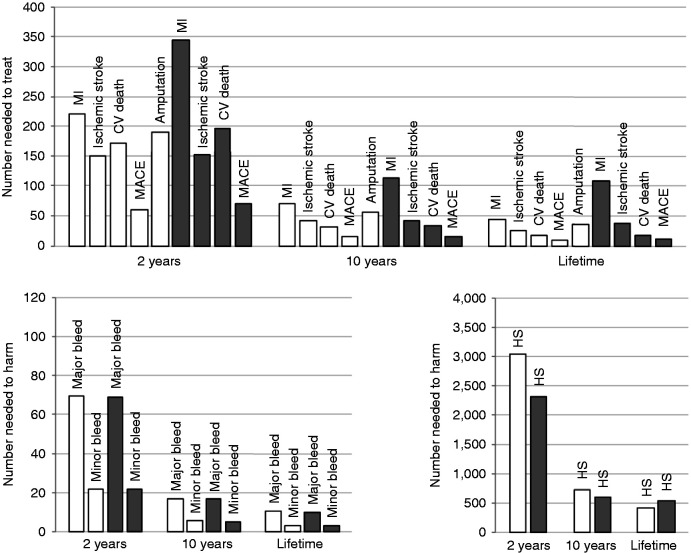
Lifelong preventive treatment of coronary artery disease and peripheral arterial disease patients at risk of cardiovascular events with dual pathway inhibition improves health outcomes and seems overall cost-effective relative to aspirin antiplatelet therapy and also to clopidogrel antiplatelet therapy for peripheral arterial disease, particularly in comorbid patients, but not in older patients and in carotid artery disease patients. These findings may warrant a targeted approach.
对于患有冠状动脉疾病和/或外周动脉疾病的患者,每日两次服用 2.5 毫克利伐沙班联合每日一次服用 100 毫克阿司匹林的双联通路抑制可能是一种有前途的替代 100 毫克阿司匹林抗血小板治疗以预防心血管事件的方法。然而,治疗费用和出血风险更高,并且外周动脉疾病还有另一种治疗选择,即 75 毫克氯吡格雷。需要对双联通路抑制与标准治疗相比的获益、风险和成本进行全面评估。
我们使用包括心血管、缺血性肢体和出血事件在内的状态转移模型,比较了双联通路抑制与冠状动脉疾病患者的阿司匹林抗血小板治疗,以及外周动脉疾病患者的氯吡格雷抗血小板治疗。我们根据终生治疗的成本和质量调整生命年来计算增量成本效果比,并以 50,000 欧元/质量调整生命年的阈值计算成本效果概率。
双联通路抑制的质量调整生命年和成本最高,与阿司匹林相比,其增量成本效果比在冠状动脉疾病患者中为 32,109 欧元,在外周动脉疾病患者中为 26,381 欧元,其成本效果概率分别为 92%和 56%(氯吡格雷被广泛地排除)。在患有合并症的外周动脉疾病患者和年龄小于 65 岁的冠状动脉疾病患者中,增量成本效果比低于 20,000 欧元,在患有颈动脉疾病患者和年龄大于 75 岁的冠状动脉疾病患者中,增量成本效果比高于 50,000 欧元。
对于有心血管事件风险的冠状动脉疾病和外周动脉疾病患者,终生预防性使用双联通路抑制可改善健康结果,并且相对于阿司匹林抗血小板治疗以及氯吡格雷抗血小板治疗(对于外周动脉疾病),总体上具有成本效果,特别是在合并症患者中,但对于老年患者和颈动脉疾病患者则不然。这些发现可能需要采取有针对性的方法。