Carmont Michael R, Zellers Jennifer A, Brorsson Annelie, Nilsson-Helander Katarina, Karlsson Jón, Grävare Silbernagel Karin
Department of Trauma and Orthopaedic Surgery, Princess Royal Hospital, Shrewsbury and Telford Hospital NHS Trust, Shropshire, UK.
Program in Physical Therapy, Washington University School of Medicine in St. Louis, St. Louis, Missouri, USA.
Orthop J Sports Med. 2020 Mar 25;8(3):2325967120909556. doi: 10.1177/2325967120909556. eCollection 2020 Mar.
Achilles tendon rupture leads to weakness of ankle plantarflexion. Treatment of Achilles tendon rupture should aim to restore function while minimizing weakness and complications of management.
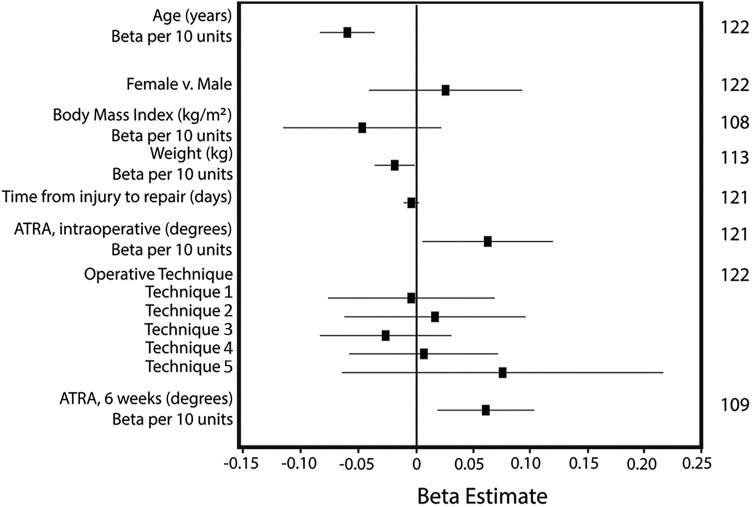
To determine the influence of factors (age, sex, body mass index [BMI], weight, time from injury to operative repair, and tightness of repair) in the initial surgical management of patients after an acute Achilles tendon rupture on 12-month functional outcome assessment after percutaneous and minimally invasive repair.
Cohort study; Level of evidence, 3.
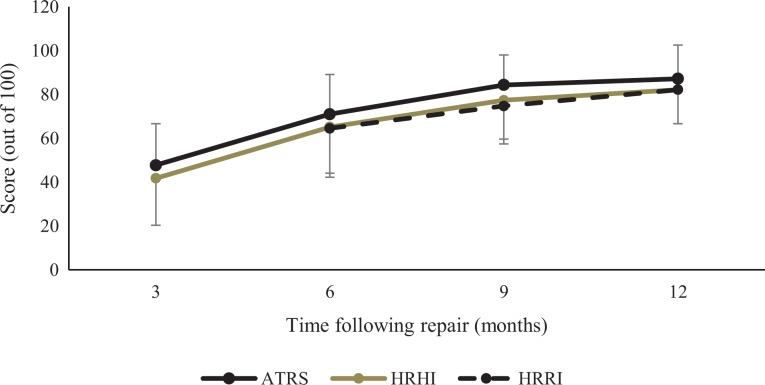
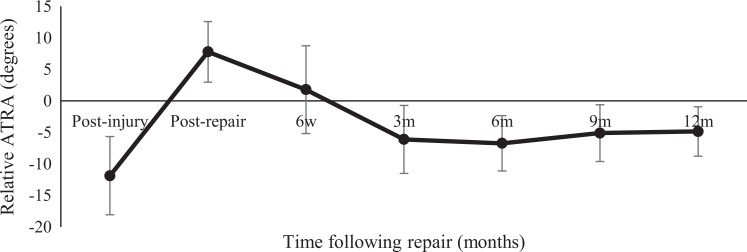
From May 2012 to January 2018, patients sustaining an Achilles tendon rupture receiving operative repair were prospectively evaluated. Tightness of repair was quantified using the intraoperative Achilles tendon resting angle (ATRA). Heel-rise height index (HRHI) was used as the primary 12-month outcome variable. Secondary outcome measures included Achilles tendon total rupture score (ATRS) and Tegner score. Stepwise multiple regression was used to create a model to predict 12-month HRHI.
A total of 122 patients met the inclusion criteria for data analysis (mean ± SD age, 44.1 ± 10.8 years; 78% male; mean ± SD BMI, 28.1 ± 4.3 kg/m). The elapsed time to surgery was 6.5 ± 4.0 days. At 12-month follow-up, patients had an HRHI of 82% ± 16% and performed 82% ± 17% of repetitions compared with the noninjured side. Participants had a mean ATRS of 87 ± 15 and a median Tegner score of 5 (range, 1-9), with a reduction in Tegner score of 2 from preinjury levels. The relative ATRA at 12 months was -4.8° ± 3.9°. Multiple regression identified younger age (B = ±0.006; < .001) and greater intraoperative ATRA (B = 0.005; = .053) as predictors of more symmetrical 12-month HRHI ( = 0.19; < .001; n = 120).
Age was found to be the strongest predictor of outcome after Achilles tendon rupture. The most important modifiable risk factor was the tightness of repair. It is recommended that repair be performed as tight as possible to optimize heel-rise height 1 year after Achilles tendon rupture and possibly to reduce tendon elongation.
跟腱断裂会导致踝关节跖屈无力。跟腱断裂的治疗应旨在恢复功能,同时将管理的无力和并发症降至最低。
确定急性跟腱断裂患者初次手术治疗中的因素(年龄、性别、体重指数[BMI]、体重、受伤至手术修复的时间以及修复的紧密度)对经皮和微创修复后12个月功能结局评估的影响。
队列研究;证据等级,3级。
对2012年5月至2018年1月接受手术修复的跟腱断裂患者进行前瞻性评估。使用术中跟腱静息角(ATRA)对修复的紧密度进行量化。足跟抬高高度指数(HRHI)用作12个月的主要结局变量。次要结局指标包括跟腱完全断裂评分(ATRS)和特格纳评分。采用逐步多元回归建立预测12个月HRHI的模型。
共有122例患者符合数据分析的纳入标准(平均±标准差年龄,44.1±10.8岁;78%为男性;平均±标准差BMI,28.1±4.3kg/m)。手术 elapsed 时间为6.5±4.0天。在12个月随访时,患者的HRHI为82%±16%,与未受伤侧相比,重复次数为82%±17%。参与者的平均ATRS为87±15,特格纳评分中位数为5(范围,1 - 9),与受伤前水平相比,特格纳评分降低了2分。12个月时的相对ATRA为 -4.8°±3.9°。多元回归确定年龄较小(B = ±0.006;P <.001)和术中ATRA较大(B = 0.005;P =.053)是12个月HRHI更对称的预测因素(R² = 0.19;P <.001;n = 120)。
年龄被发现是跟腱断裂后结局的最强预测因素。最重要的可改变风险因素是修复的紧密度。建议尽可能紧密地进行修复,以优化跟腱断裂1年后的足跟抬高高度,并可能减少肌腱伸长。