Behavioral Pharmacology Research Unit, Johns Hopkins University School of Medicine, 5510 Nathan Shock Dr., Baltimore, MD, 21224, USA.
Behavioral Pharmacology Research Unit, Johns Hopkins University School of Medicine, 5510 Nathan Shock Dr., Baltimore, MD, 21224, USA.
Drug Alcohol Depend. 2020 Jun 1;211:107937. doi: 10.1016/j.drugalcdep.2020.107937. Epub 2020 Apr 1.
The use and availability of oral and inhalable products containing cannabidiol (CBD) as the principal constituent has increased with expanded cannabis/hemp legalization. However, few controlled clinical laboratory studies have evaluated the pharmacodynamic effects of oral or vaporized CBD or CBD-dominant cannabis.
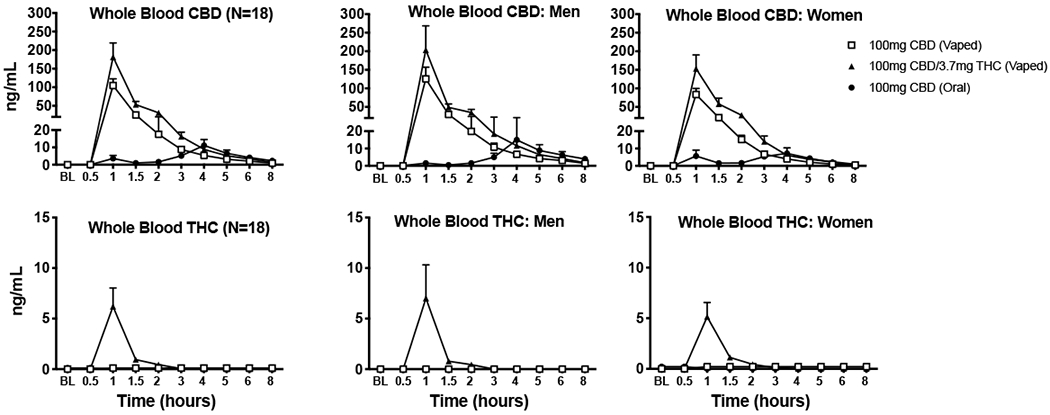
Eighteen healthy adults (9 men; 9 women) completed four, double-blind, double-dummy, drug administration sessions. Sessions were separated by ≥1 week and included self-administration of 100 mg oral CBD, 100 mg vaporized CBD, vaporized CBD-dominant cannabis (100 mg CBD; 3.7 mg THC), and placebo. Study outcomes included: subjective drug effects, vital signs, cognitive/psychomotor performance, and whole blood THC and CBD concentrations.
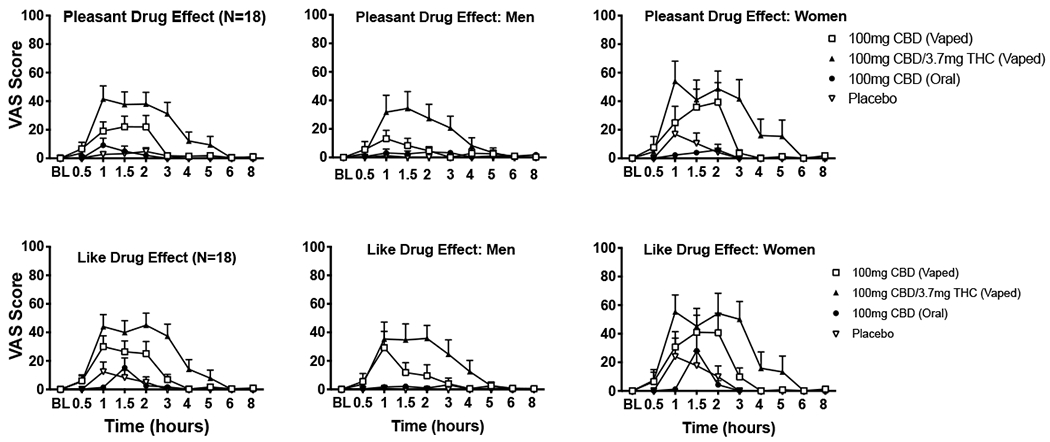
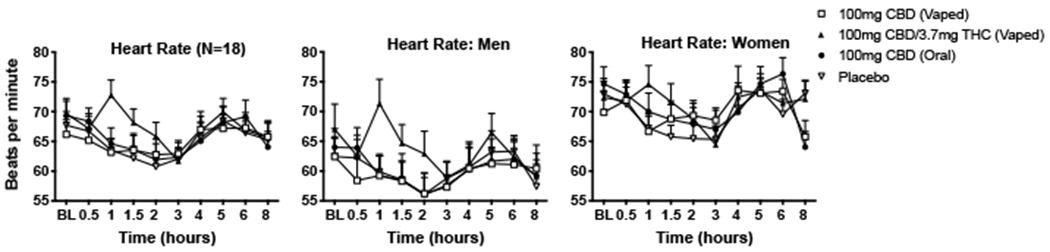
Vaporized CBD and CBD-dominant cannabis increased ratings on several subjective items (e.g., Like Drug Effect) relative to placebo. Subjective effects did not differ between oral CBD and placebo and were generally higher for CBD-dominant cannabis compared to vaporized CBD. CBD did not increase ratings for several items typically associated with acute cannabis/THC exposure (e.g., Paranoid). Women reported qualitatively higher ratings for Pleasant Drug Effect than men after vaporized CBD and CBD-dominant cannabis use. CBD-dominant cannabis increased heart rate compared to placebo. Cognitive/psychomotor impairment was not observed in any drug condition.
Vaporized CBD and CBD-dominant cannabis produced discriminable subjective drug effects, which were sometimes stronger in women, but did not produce cognitive/psychomotor impairment. Subjective effects of oral CBD did not differ from placebo. Future research should further elucidate the subjective effects of various types of CBD products (e.g., inhaled, oral, topical), which appear to be distinct from THC-dominant products.
随着大麻/大麻合法化的扩大,含有大麻二酚 (CBD) 作为主要成分的口服和吸入产品的使用和供应有所增加。然而,很少有对照临床实验室研究评估过口服或雾化 CBD 或 CBD 占主导地位的大麻的药效学效应。
18 名健康成年人(9 名男性;9 名女性)完成了四次双盲、双模拟、药物给药疗程。疗程间隔至少 1 周,包括自行服用 100mg 口服 CBD、100mg 雾化 CBD、雾化 CBD 占主导地位的大麻(100mg CBD;3.7mg THC)和安慰剂。研究结果包括:主观药物效应、生命体征、认知/精神运动表现以及全血 THC 和 CBD 浓度。
与安慰剂相比,雾化 CBD 和 CBD 占主导地位的大麻增加了几个主观项目的评分(例如,喜欢药物效应)。口服 CBD 与安慰剂相比,主观效应没有差异,而 CBD 占主导地位的大麻与雾化 CBD 相比,主观效应通常更高。CBD 没有增加几个通常与急性大麻/THC 暴露相关的项目的评分(例如,偏执)。与使用雾化 CBD 和 CBD 占主导地位的大麻后相比,女性报告的愉快药物效应评分明显更高。与安慰剂相比,CBD 占主导地位的大麻增加了心率。在任何药物条件下都没有观察到认知/精神运动损伤。
雾化 CBD 和 CBD 占主导地位的大麻产生了可区分的主观药物效应,在女性中有时更强,但没有产生认知/精神运动损伤。口服 CBD 的主观效应与安慰剂没有差异。未来的研究应该进一步阐明各种类型的 CBD 产品(例如,吸入、口服、局部)的主观效应,这些产品似乎与 THC 占主导地位的产品不同。