Engbers Aline G J, Flint Robert B, Völler Swantje, de Klerk Johan C A, Reiss Irwin K M, Andriessen Peter, Liem Kian D, Degraeuwe Pieter L J, Croubels Siska, Millecam Joske, Allegaert Karel, Simons Sinno H P, Knibbe Catherijne A J
Division of Systems Biomedicine & Pharmacology, LACDR, Leiden University, Leiden, the Netherlands.
Department of Paediatrics, Division of Neonatology, Erasmus UMC - Sophia Children's Hospital, Rotterdam, the Netherlands.
Br J Clin Pharmacol. 2020 Oct;86(10):2028-2039. doi: 10.1111/bcp.14298. Epub 2020 Apr 20.
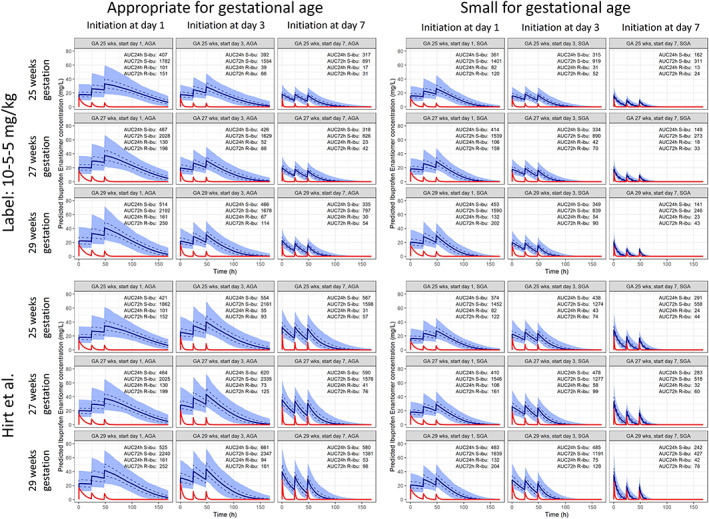
Racemic ibuprofen is widely used for the treatment of preterm neonates with patent ductus arteriosus. Currently used bodyweight-based dosing guidelines are based on total ibuprofen, while only the S-enantiomer of ibuprofen is pharmacologically active. We aimed to optimize ibuprofen dosing for preterm neonates of different ages based on an enantiomer-specific population pharmacokinetic model.
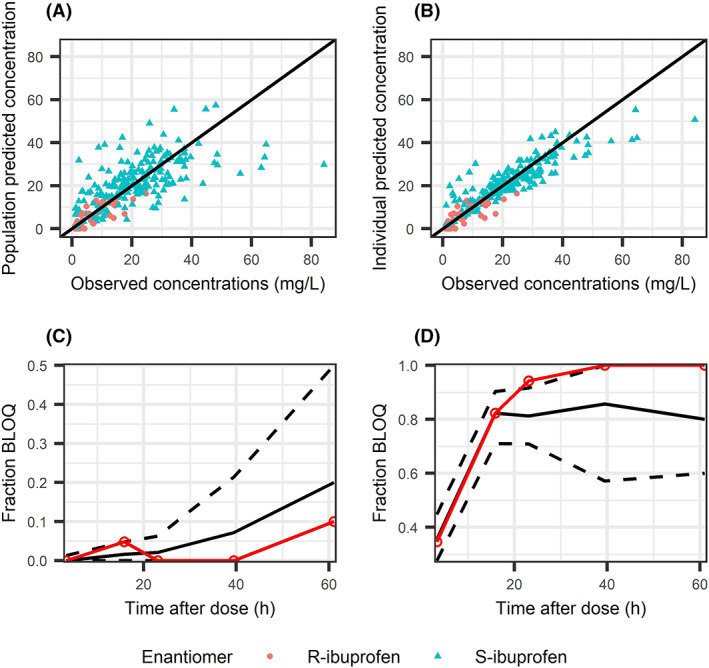
We prospectively collected 210 plasma samples of 67 preterm neonates treated with ibuprofen for patent ductus arteriosus (median gestational age [GA] 26 [range 24-30] weeks, median body weight 0.83 [0.45-1.59] kg, median postnatal age [PNA] 3 [1-12] days), and developed a population pharmacokinetic model for S- and R-ibuprofen.
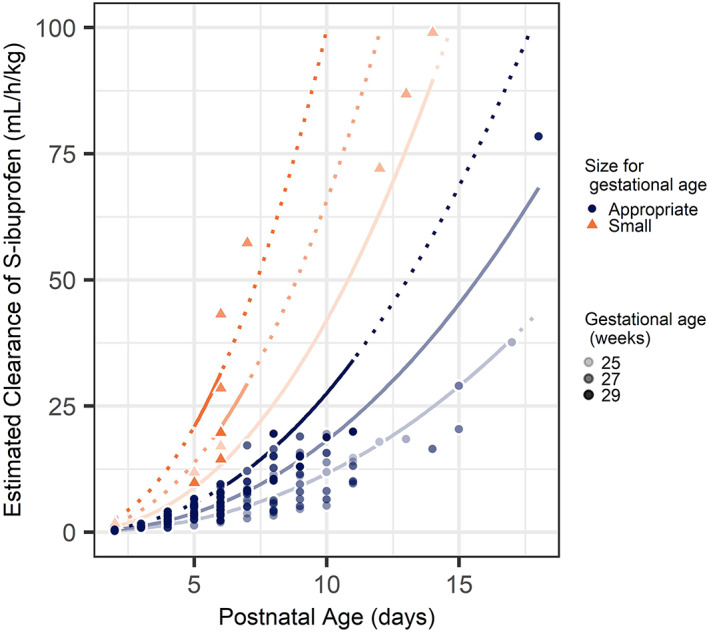
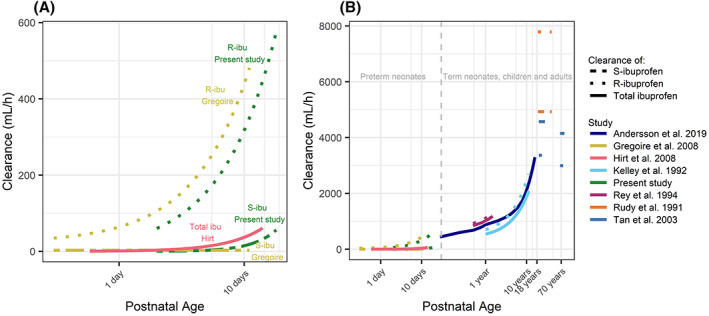
We found that S-ibuprofen clearance (CL , 3.98 mL/h [relative standard error {RSE} 8%]) increases with PNA and GA, with exponents of 2.25 (RSE 6%) and 5.81 (RSE 15%), respectively. Additionally, a 3.11-fold higher CL was estimated for preterm neonates born small for GA (RSE 34%). Clearance of R-ibuprofen was found to be high compared to CL (18 mL/h [RSE 24%]), resulting in a low contribution of R-ibuprofen to total ibuprofen exposure. Current body weight was identified as covariate on both volume of distribution of S-ibuprofen and R-ibuprofen.
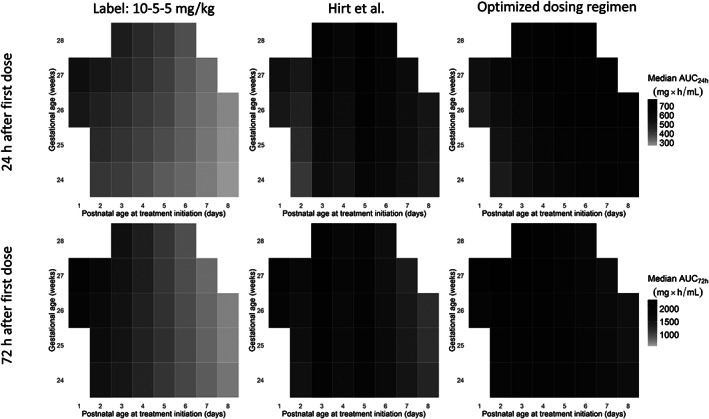
S-ibuprofen clearance shows important maturation, especially with PNA, resulting in an up to 3-fold increase in CL during a 3-day treatment regimen. This rapid increase in clearance needs to be incorporated in dosing guidelines by adjusting the dose for every day after birth to achieve equal ibuprofen exposure.
消旋布洛芬广泛用于治疗患有动脉导管未闭的早产儿。目前使用的基于体重的给药指南是基于布洛芬总量,而只有布洛芬的S-对映体具有药理活性。我们旨在基于对映体特异性群体药代动力学模型优化不同年龄早产儿的布洛芬给药方案。
我们前瞻性收集了67例接受布洛芬治疗动脉导管未闭的早产儿的210份血浆样本(中位胎龄[GA]26[范围24 - 30]周,中位体重0.83[0.45 - 1.59]kg,中位出生后年龄[PNA]3[1 - 12]天),并建立了S-和R-布洛芬的群体药代动力学模型。
我们发现S-布洛芬清除率(CL,3.98 mL/h[相对标准误差{RSE}8%])随PNA和GA增加,指数分别为2.25(RSE 6%)和5.81(RSE 15%)。此外,对于小于胎龄儿出生的早产儿,估计CL高3.11倍(RSE 34%)。发现R-布洛芬的清除率与CL相比很高(18 mL/h[RSE 24%]),导致R-布洛芬对总布洛芬暴露的贡献较低。当前体重被确定为S-布洛芬和R-布洛芬分布容积的协变量。
S-布洛芬清除率显示出重要的成熟过程,尤其是随PNA,在为期3天的治疗方案中导致CL增加高达3倍。这种清除率的快速增加需要纳入给药指南,通过调整出生后每天的剂量以实现相等的布洛芬暴露。