Sun Yat-sen University Cancer Center, 651 Dongfeng Road, East, Guangzhou, 510060, China.
State Key Laboratory of Oncology in South China, 651 Dongfeng Road, East, Guangzhou, 510060, China.
Cancer Imaging. 2020 Apr 6;20(1):25. doi: 10.1186/s40644-020-00299-x.
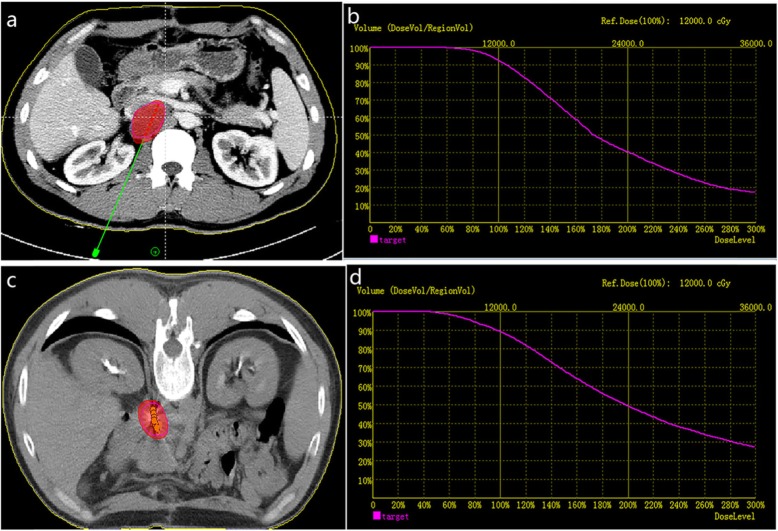
Due to the unique anatomical location of retroperitoneal metastatic lymph nodes, current treatment options are limited. This study was designed to explore the clinical efficacy and prognostic factors of CT-guided I brachytherapy for the treatment of retroperitoneal metastatic lymph nodes.
We retrospectively evaluated 92 patients received I brachytherapy for retroperitoneal metastatic lymph nodes. A layered Cox proportional hazards model was established to filter out the independent factors affecting local tumor progression-free survival (LTPFS).
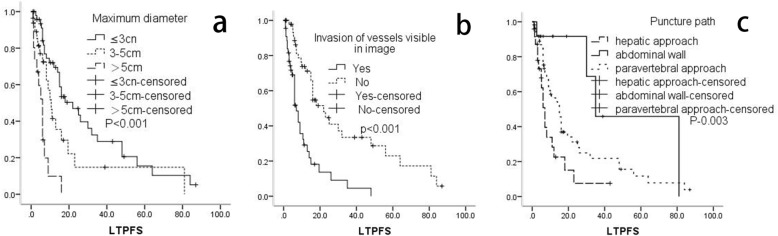
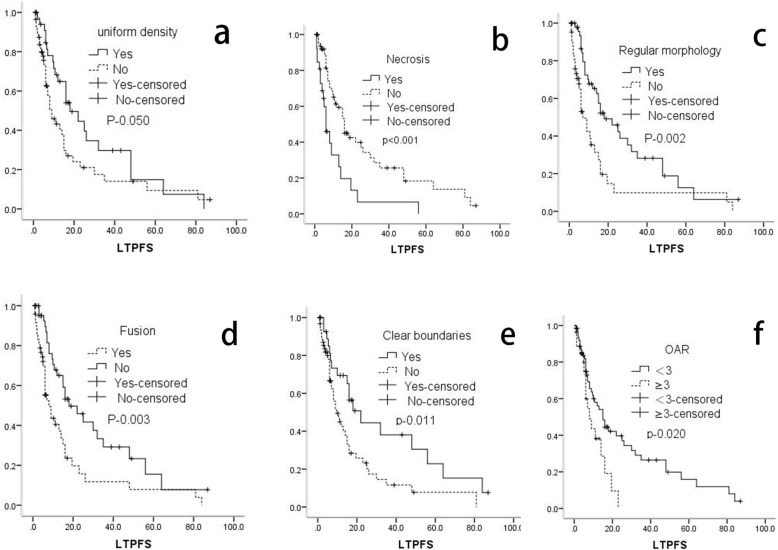
The median LTPFS was 8 months. Metastatic lymph node with uniform density (p-0.009), clear boundaries (p-0.011), regular morphology (P < 0.001), and < 3 organs at risk of metastasis (p-0.020) were associated with better LTPFS. Necrotic lymph nodes (p < 0.001), fusion (p-0.003), and invasion of vessels visible on images (p < 0.001) were associated with poor LTPFS. Puncture path through abdominal wall or paravertebral approach were also associated with better LTPFS than a hepatic approach (P < 0.05). A maximum diameter ≤ 3 cm (P-0.031) or 3-5 cm (P-0.018) were also associated with significantly better LTPFS than a maximum diameter ≥ 5 cm. The Cox proportional hazards model suggested that lymph nodes invaded the large vessels visible on images, maximum diameter and puncture path were independent risk factors for LTPFS.
CT-guided I brachytherapy is an optional palliative treatment modality for retroperitoneal metastatic lymph nodes, which can provide high local control without severe complications. Better preoperative planning, intraoperative implementation, better choice of puncture path, and selection of appropriate tumor size are important factors that can improve the clinical efficacy of I brachytherapy for retroperitoneal metastatic lymph nodes.
由于腹膜后转移性淋巴结的独特解剖位置,目前的治疗选择有限。本研究旨在探讨 CT 引导下 I 近距离放疗治疗腹膜后转移性淋巴结的临床疗效和预后因素。
我们回顾性评估了 92 例接受 I 近距离放疗治疗腹膜后转移性淋巴结的患者。建立分层 Cox 比例风险模型,筛选影响局部肿瘤无进展生存期(LTPFS)的独立因素。
中位 LTPFS 为 8 个月。具有均匀密度(p-0.009)、清晰边界(p-0.011)、规则形态(P<0.001)和<3 个转移风险器官的转移性淋巴结(p-0.020)与更好的 LTPFS 相关。坏死淋巴结(p<0.001)、融合(p-0.003)和图像上可见血管侵犯(p<0.001)与较差的 LTPFS 相关。经腹壁或椎旁途径的穿刺路径也比经肝途径(P<0.05)与更好的 LTPFS 相关。最大直径≤3cm(P-0.031)或 3-5cm(P-0.018)也与显著更好的 LTPFS 相关,最大直径≥5cm。Cox 比例风险模型提示,图像上可见大血管侵犯、最大直径和穿刺路径是 LTPFS 的独立危险因素。
CT 引导下 I 近距离放疗是腹膜后转移性淋巴结的一种可选的姑息性治疗方法,可提供高局部控制率而无严重并发症。更好的术前规划、术中实施、更好的穿刺路径选择和适当的肿瘤大小选择是提高 I 近距离放疗治疗腹膜后转移性淋巴结的临床疗效的重要因素。