González-Cordero Gustavo, Garduño-Chávez Belia Inés, Palacios-Ríos Dionisio, Estrada-Solís Yesenia Nohemí, Rodríguez-Sánchez Iram Pablo, Martínez-Ponce-de-León Ángel Raymundo
Servicio de Anestesiología, Universidad Autónoma de Nuevo León, Facultad de Medicina y Hospital Universitario 'Dr Jose Eleuterio Gonzalez, Monterrey, Nuevo León 64460, Mexico.
Laboratorio de Fisiología Molecular y Estructural, Universidad Autónoma de Nuevo León, Facultad de Ciencias Biológicas, San Nicolás de los Garza, Nuevo León 66450, Mexico.
Exp Ther Med. 2020 Apr;19(4):2563-2569. doi: 10.3892/etm.2020.8507. Epub 2020 Feb 10.
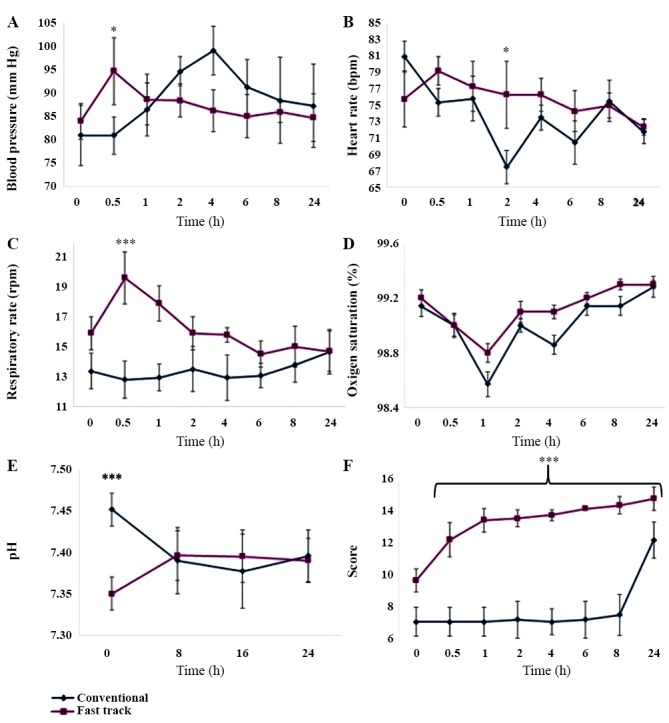
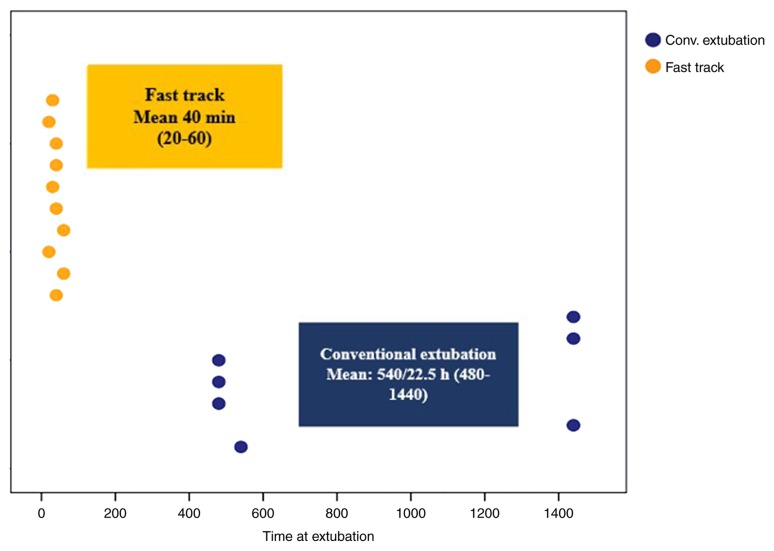
Early extubation, also known as fast track, is desirable after intracranial hematoma surgery to avoid ventilator-associated complications associated with admission to an intensive care unit (ICU). The objective of the present study was to determine whether ICU stay and ventilator-associated complications are reduced in patients who received surgery for intracranial hematoma if they are extubated early. A total of 17 patients were randomly assigned to two groups: In Group 1, patients were extubated early or using the fast track method, while those in Group 2 were conventionally extubated at a later stage and were managed at the ICU. Patients from both groups were assessed on admission to the operating room per the established standards and after the selection criteria had been confirmed, general anesthesia was applied. Extubation time and hemodynamic stability (number of anesthetic adjustments required to maintain hemodynamic parameters within 20% of the predicted values) were assessed post-operatively. Patients in the conventional group (n=10) were transferred to the ICU and extubated at 8 h post-operatively; hemodynamic stability and the presence of complications were evaluated. The fast track group had no complications associated with ventilation or any other parameter. All patients extubated in a conventional manner and who were transferred to the ICU presented with complications, including seizures, aspiration, atelectasis or failed extubation. In the future, fast track should be regarded as a routine technique in patients who meet the required criteria, so that they may be discharged quickly and with fewer complications. The present study was authorized by the ethics committee of the hospital and the research sub-directorate with the number AN14-003; it was submitted to and approved by the ISRCTN registry for clinical trials (ID, ISRCTN16924441).
早期拔管,也称为快速康复,在颅内血肿手术后是可取的,以避免与入住重症监护病房(ICU)相关的呼吸机相关并发症。本研究的目的是确定颅内血肿手术患者早期拔管是否能减少ICU住院时间和呼吸机相关并发症。总共17例患者被随机分为两组:在第1组中,患者早期拔管或采用快速康复方法,而第2组患者则在后期进行传统拔管并在ICU进行管理。两组患者在进入手术室时均按照既定标准进行评估,在确认入选标准后,实施全身麻醉。术后评估拔管时间和血流动力学稳定性(将血流动力学参数维持在预测值的20%以内所需的麻醉调整次数)。传统组(n = 10)的患者被转移到ICU,并在术后8小时拔管;评估血流动力学稳定性和并发症的发生情况。快速康复组没有与通气或任何其他参数相关的并发症。所有以传统方式拔管并被转移到ICU的患者均出现并发症,包括癫痫发作、误吸、肺不张或拔管失败。未来,对于符合要求标准的患者,快速康复应被视为一种常规技术,以便他们能够更快出院且并发症更少。本研究得到了医院伦理委员会和研究分部门的批准,编号为AN14 - 003;它已提交给ISRCTN临床试验注册中心并获得批准(注册号,ISRCTN16924441)。