Liu Jing, Huang Xinhua, Hu Siping, Meng Zhipeng, He Huanzhong
Department of Anesthesiology, Huzhou Maternity and Child Healthcare Hospital, Huzhou, Zhejiang 313000, P.R. China.
Department of Anesthesiology, Huzhou Central Hospital, Affiliated Central Hospital of Huzhou University, Huzhou, Zhejiang 313000, P.R. China.
Exp Ther Med. 2020 Apr;19(4):3051-3059. doi: 10.3892/etm.2020.8549. Epub 2020 Feb 25.
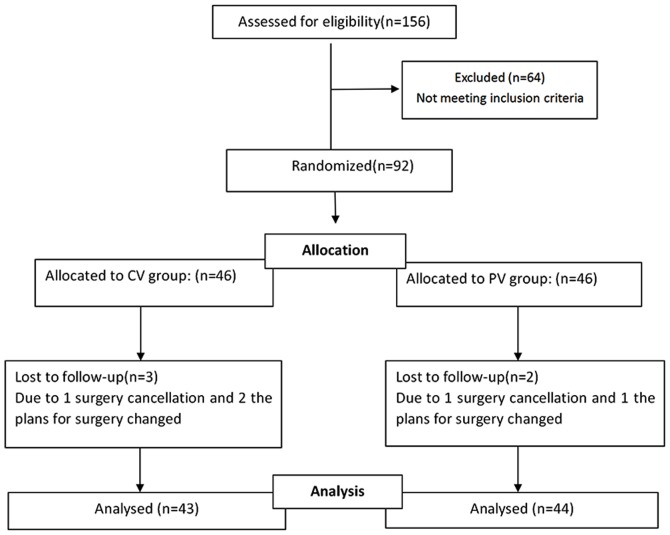
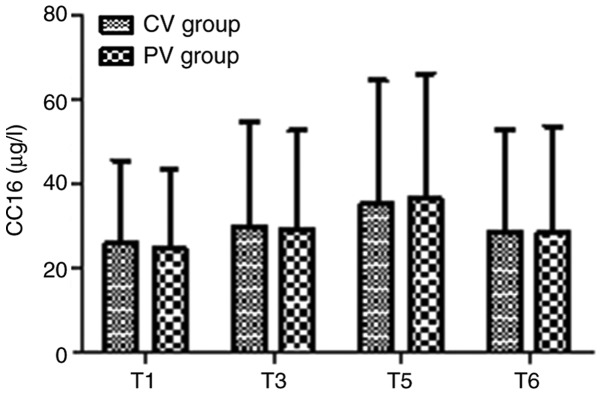
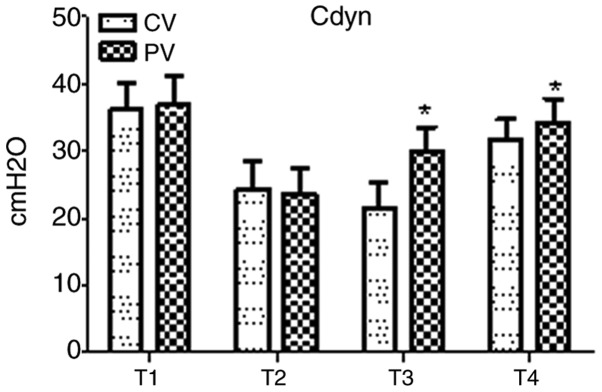
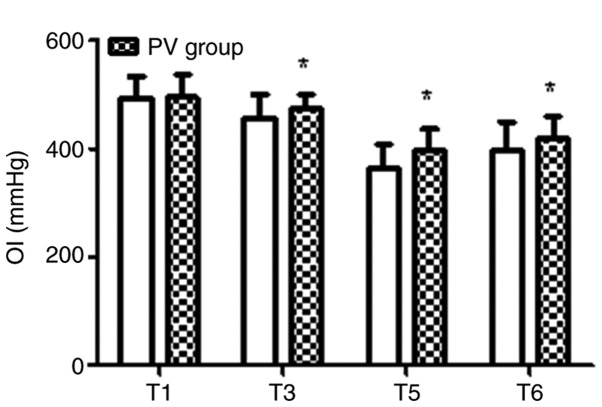
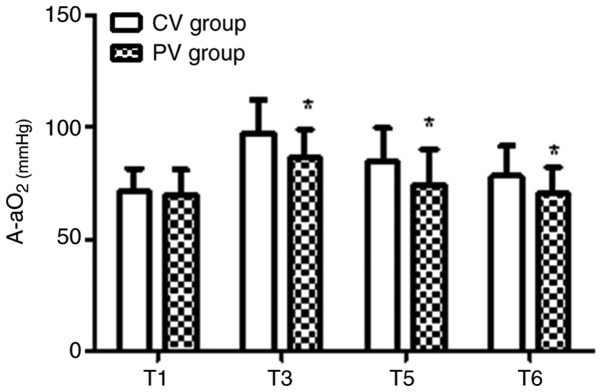
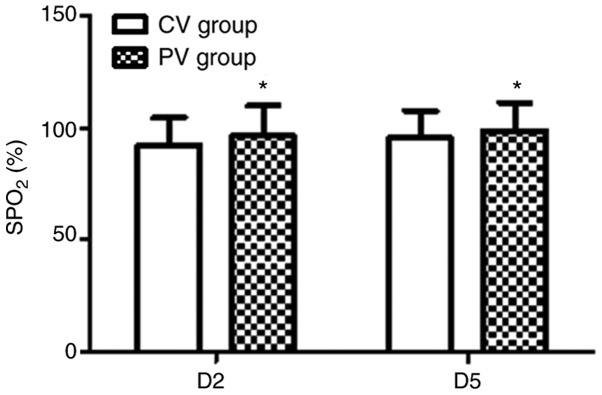
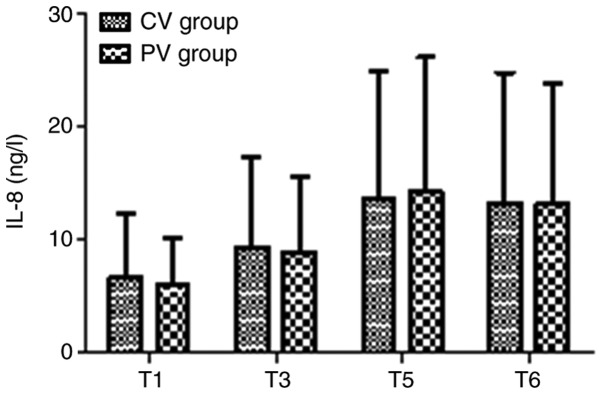
Laparoscopic total hysterectomy is performed by carbon dioxide insufflation, Trendelenburg position and mechanical ventilation of patients under general anesthesia. However, this may induce pulmonary atelectasis and/or hyperdistention of the lungs. Multiple studies have indicated that mechanical ventilation with the use of low tidal volumes, moderate positive end-expiratory pressure (PEEP) and regular alveolar recruitment maneuvers may improve post-operative outcomes. However, the benefits of an individualized level of PEEP have not been clearly established. In the present study, it was hypothesized that a moderate fixed PEEP may not suit all patients and an individually-titrated PEEP during anesthesia may improve the peri-operative pulmonary oxygenation function. The aim of the present study was to compare the pulmonary oxygenation function and post-operative pulmonary complications (PPCs) in patients receiving individualized lung-protective mechanical ventilation (LPV) vs. conventional ventilation (CV) during laparoscopic total hysterectomy. The present study was a randomized double-blinded clinical trial on 87 patients who were randomly divided to receive CV or protective ventilation (PV). An optimal individualized PEEP value was determined using a static pulmonary compliance-directed PEEP titration procedure. Pulmonary oxygenation function, serum inflammatory factors, including interleukin-8 and Clara cell protein 16, the incidence of PPCs and the post-operative length of stay were also determined. Patients in the PV group exhibited improved pulmonary oxygenation function during and after the operation. The total percentage of PPCs during the first 7 days after surgery was significantly lower in the PV group compared with those in the CV group. In conclusion, as compared to CV, intra-operative individualized LPV significantly improved pulmonary oxygenation function and reduced the incidence of PPCs during the first 7 days after laparoscopic total hysterectomy (Clinical trial registration no. ChiCTR1900027738).
腹腔镜全子宫切除术是在全身麻醉下通过二氧化碳气腹、头低脚高位及机械通气对患者进行的。然而,这可能会导致肺不张和/或肺过度膨胀。多项研究表明,采用低潮气量、适度呼气末正压(PEEP)和常规肺泡复张手法进行机械通气可能会改善术后结局。然而,个体化PEEP水平的益处尚未明确确立。在本研究中,我们假设适度固定的PEEP可能并不适合所有患者,麻醉期间个体化滴定的PEEP可能会改善围手术期肺氧合功能。本研究的目的是比较腹腔镜全子宫切除术期间接受个体化肺保护性机械通气(LPV)与传统通气(CV)的患者的肺氧合功能和术后肺部并发症(PPCs)。本研究是一项针对87例患者的随机双盲临床试验,这些患者被随机分为接受CV或保护性通气(PV)。使用静态肺顺应性导向的PEEP滴定程序确定最佳个体化PEEP值。还测定了肺氧合功能、血清炎症因子,包括白细胞介素-8和克拉拉细胞蛋白16、PPCs的发生率和术后住院时间。PV组患者在手术期间和术后肺氧合功能均得到改善。与CV组相比,PV组术后第1个7天内PPCs的总发生率显著降低。总之,与CV相比,术中个体化LPV显著改善了肺氧合功能,并降低了腹腔镜全子宫切除术后第1个7天内PPCs的发生率(临床试验注册号:ChiCTR19000