Geisel School of Medicine at Dartmouth, Hanover, New Hampshire, USA.
Harvard Medical School, Boston, Massachusetts, USA.
J Glob Health. 2020 Jun;10(1):010407. doi: 10.7189/jogh.10.010407.
Cardiovascular disease (CVD) morbidity and mortality are increasing in sub-Saharan Africa (sSA), highlighting the need for tools to enable CVD risk stratification in the region. Although non-HDL-cholesterol (nHDL-C) has been promoted as a method to measure lipids without a requirement for fasting in the USA, its diagnostic validity has not been assessed in sSA. We sought to estimate: 1) the association between LDL-cholesterol (LDL-C) and nHDL-C, 2) the impact of fasting on their measurement, and 3) their correlation with carotid atherosclerosis, within a rural Ugandan population with high HIV prevalence.
We collected traditional CVD risk factors, blood for serum lipid levels, self-reported fasting status, and performed carotid ultrasonography in 301 participants in rural Uganda. We fit regression models, stratified by fasting status, to estimate associations between carotid intima media thickness (cIMT), LDL-C, and nHDL-C.
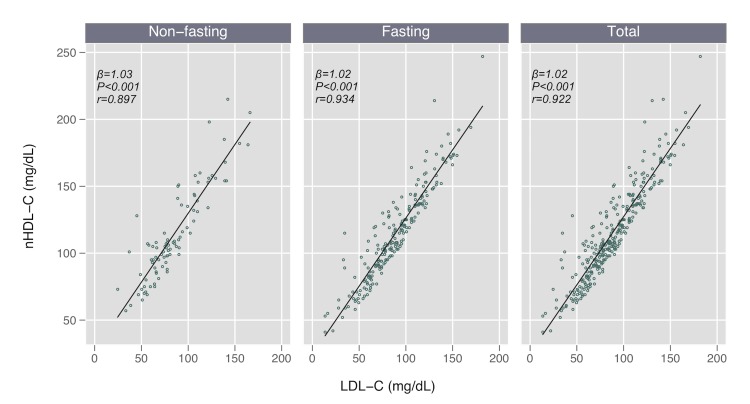
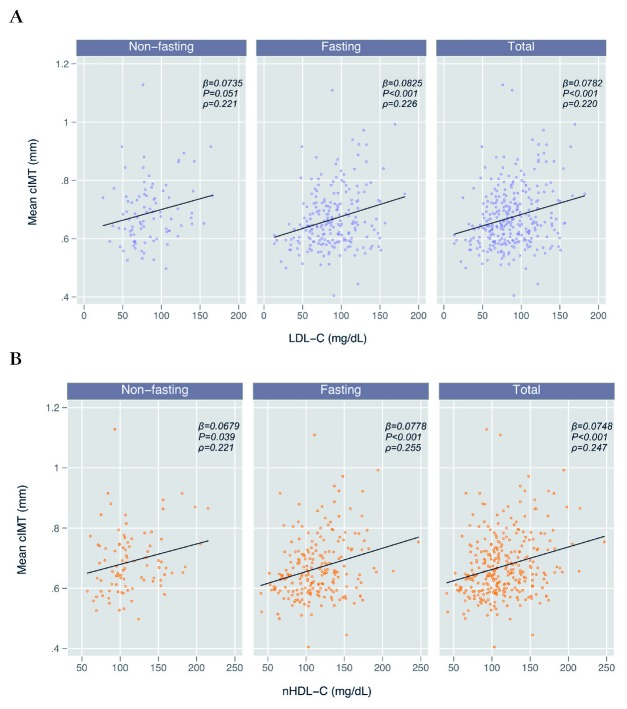
Median age was 50 years (interquartile range = 46-54), 49% were female, 51% were HIV-positive, and at the time of blood collection, 70% had fasted overnight. Mean LDL-C, nHDL-C, and triglycerides in the non-fasting and fasting groups were 85 vs 88 mg/dL ( = 0.39), 114 vs 114 mg/dL ( = 0.98), and 130 vs 114 mg/dL ( = 0.05) mg/dL, respectively. In unadjusted models, mean cIMT (mm) was associated with both increased LDL-C (β = 0.0078 per 10mg/dL, < 0.01) and nHDL-C (β = 0.0075, < 0.01), and these relationships were similar irrespective of fasting status. After adjustment for traditional CVD risk factors, we observed similar associations, albeit with muted effect sizes within the fasting group.
We found a high correlation between LDL-C and nHDL-C, and both were correlated with cIMT, irrespective of fasting or HIV serostatus in rural Uganda. Our findings support use of either fasting or non-fasting serum lipids for CVD risk estimation in rural sSA.
在撒哈拉以南非洲(sSA),心血管疾病(CVD)的发病率和死亡率正在上升,这凸显了在该地区需要工具来进行 CVD 风险分层的必要性。尽管非高密度脂蛋白胆固醇(nHDL-C)已在美国被推广为一种无需禁食即可测量脂质的方法,但尚未在 sSA 评估其诊断准确性。我们旨在评估:1)在 HIV 流行率较高的乌干达农村人群中,LDL-C 与 nHDL-C 之间的关联,2)禁食对其测量的影响,以及 3)它们与颈动脉粥样硬化的相关性。
我们收集了传统的 CVD 危险因素、血清脂质水平的血液样本以及自我报告的禁食状态,并对乌干达农村地区的 301 名参与者进行了颈动脉超声检查。我们按禁食状态分层拟合回归模型,以估计颈动脉内膜中层厚度(cIMT)、LDL-C 和 nHDL-C 之间的关联。
中位年龄为 50 岁(四分位距=46-54),49%为女性,51%为 HIV 阳性,在采血时,70%的人已经禁食过夜。非禁食组和禁食组的 LDL-C、nHDL-C 和甘油三酯的平均值分别为 85 与 88mg/dL(=0.39)、114 与 114mg/dL(=0.98)和 130 与 114mg/dL(=0.05)mg/dL。在未调整的模型中,cIMT(mm)与 LDL-C(每 10mg/dL 增加 0.0078,<0.01)和 nHDL-C(β=0.0075,<0.01)均呈正相关,且无论禁食状态如何,这些关系均相似。在调整了传统 CVD 危险因素后,我们观察到了相似的关联,但在禁食组中,效应大小有所减弱。
我们发现 LDL-C 和 nHDL-C 之间存在高度相关性,并且在乌干达农村地区,无论禁食或 HIV 血清阳性状态如何,两者均与 cIMT 相关。我们的研究结果支持在农村 sSA 使用禁食或非禁食血清脂质进行 CVD 风险估计。