Li Chen, Su Hai-Bin, Liu Xiao-Yan, Hu Jin-Hua
Liver Failure Treatment and Research Center, The Fifth Medical Center of Chinese PLA General Hospital, Beijing 100039, China.
World J Clin Cases. 2020 Mar 26;8(6):1042-1055. doi: 10.12998/wjcc.v8.i6.1042.
Acute-on-chronic liver failure (ACLF), which includes hepatic and multiple extra-hepatic organ failure, is a severe emergency condition that has high mortality. ACLF can rapidly progress and requires an urgent assessment of condition and referral for liver transplantation. Bacterial infections (BIs) trigger ACLF and play pivotal roles in the deterioration of clinical course.
To investigate the clinical characteristics and 28-d outcomes of first BIs either at admission or during hospitalization in patients with hepatitis B virus (HBV)-ACLF as defined by the Chinese Group on the Study of Severe Hepatitis B (COSSH).
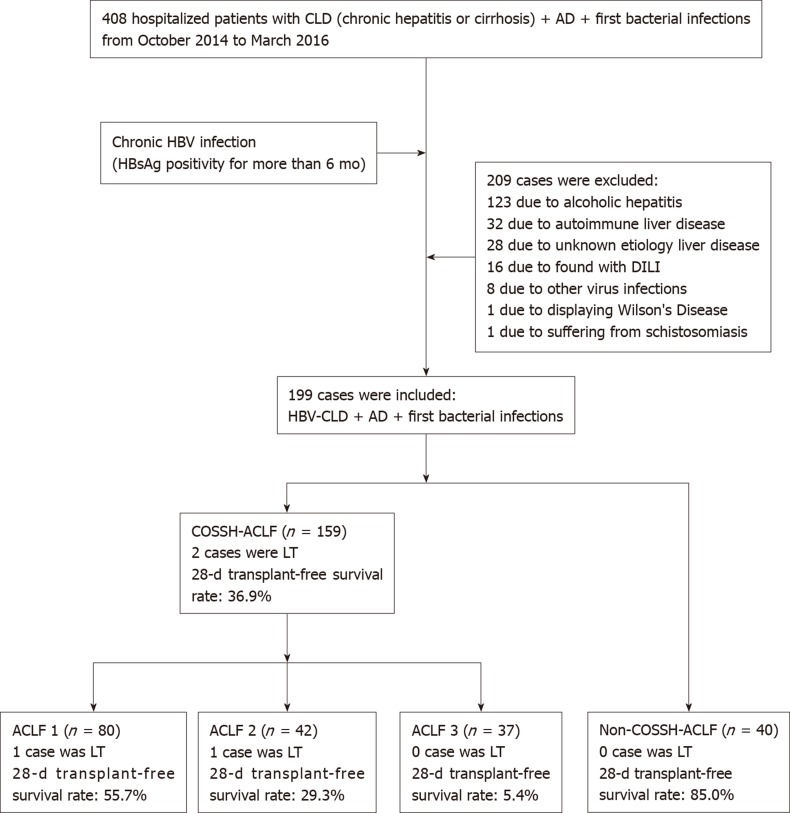
A total of 159 patients with HBV-ACLF and 40 patients with acute decompensation of HBV-related chronic liver disease combined with first BIs were selected for a retrospective analysis between October 2014 and March 2016. The characteristics of BIs, the 28-d transplant-free survival rates, and the independent predictors of the 28-d outcomes were evaluated.
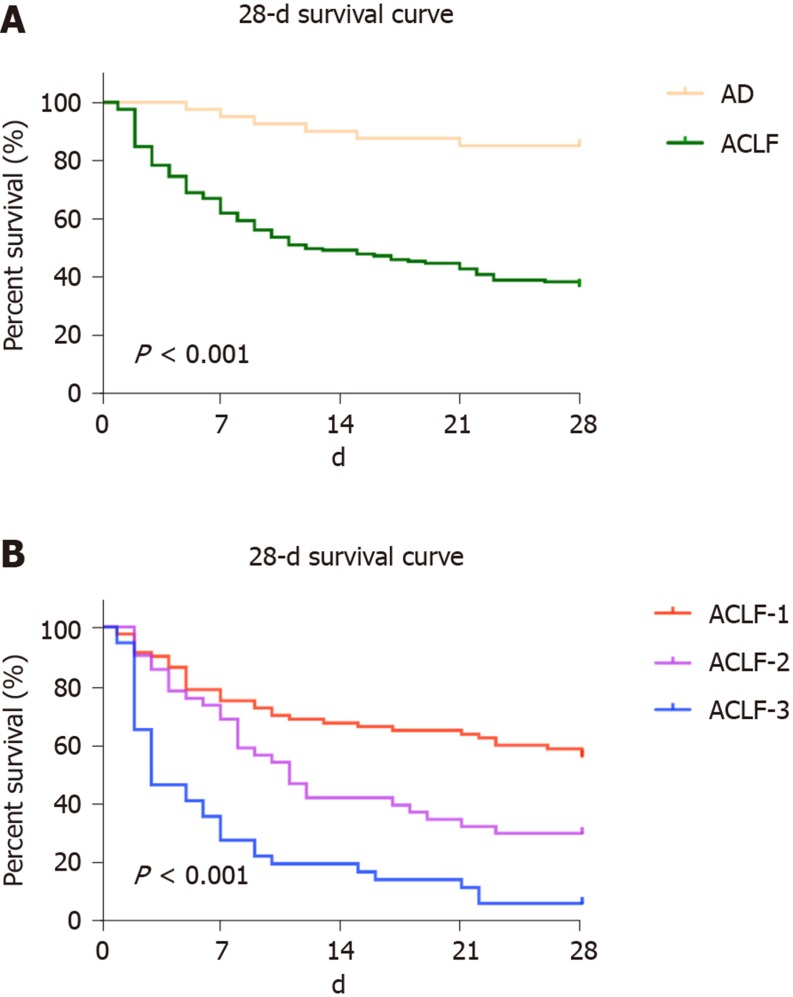
A total of 194 episodes of BIs occurred in 159 patients with HBV-ACLF. Among the episodes, 13.4% were community-acquired, 46.4% were healthcare-associated, and 40.2% belonged to nosocomial BIs. Pneumonia (40.7%), spontaneous bacterial peritonitis (SBP) (34.5%), and bloodstream infection (BSI) (13.4%) were the most prevalent. As the ACLF grade increased, the incidence of SBP showed a downward trend ( = 0.021). Sixty-one strains of bacteria, including 83.6% Gram-negative bacteria and 29.5% multidrug-resistant organisms, were cultivated from 50 patients with ACLF. (44.3%) and (23.0%) were the most common bacteria. As the ACLF grade increased, the 28-d transplant-free survival rates showed a downward trend (ACLF-1, 55.7%; ACLF-2, 29.3%; ACLF-3, 5.4%; < 0.001). The independent predictors of the 28-d outcomes of patients with HBV-ACLF were COSSH-ACLF score (hazard ratio [HR] = 1.371), acute kidney injury (HR = 2.187), BSI (HR = 2.339), prothrombin activity (HR = 0.967), and invasive catheterization (HR = 2.173).
For patients with HBV-ACLF combined with first BIs, pneumonia is the most common form, and the incidence of SBP decreases with increasing ACLF grade. COSSH-ACLF score, acute kidney injury, BSI, prothrombin activity, and invasive catheterization are the independent predictors of 28-d outcomes.
慢加急性肝衰竭(ACLF)包括肝脏及多个肝外器官衰竭,是一种死亡率很高的严重急症。ACLF可迅速进展,需要对病情进行紧急评估并转诊以进行肝移植。细菌感染(BIs)引发ACLF并在临床病程恶化中起关键作用。
调查由中国重型乙型肝炎研究组(COSSH)定义的乙型肝炎病毒(HBV)-ACLF患者入院时或住院期间首次发生BIs的临床特征及28天结局。
选取2014年10月至2016年3月期间159例HBV-ACLF患者及40例HBV相关慢性肝病急性失代偿合并首次BIs患者进行回顾性分析。评估BIs的特征、28天无移植生存率及28天结局的独立预测因素。
159例HBV-ACLF患者共发生194次BIs发作。在这些发作中,13.4%为社区获得性,46.4%为医疗相关,40.2%属于医院内BIs。肺炎(40.7%)、自发性细菌性腹膜炎(SBP)(34.5%)和血流感染(BSI)(13.4%)最为常见。随着ACLF分级增加,SBP的发生率呈下降趋势(P = 0.021)。从50例ACLF患者中培养出61株细菌,其中革兰阴性菌占83.6%,多重耐药菌占29.5%。大肠埃希菌(44.3%)和肺炎克雷伯菌(23.0%)最为常见。随着ACLF分级增加,28天无移植生存率呈下降趋势(ACLF-1级,55.7%;ACLF-2级,29.3%;ACLF-3级,5.4%;P < 0.001)。HBV-ACLF患者28天结局的独立预测因素为COSSH-ACLF评分(风险比[HR]=1.371)、急性肾损伤(HR = 2.187)、BSI(HR = 2.339)、凝血酶原活动度(HR = 0.967)及侵入性导管插入术(HR = 2.173)。
对于合并首次BIs的HBV-ACLF患者,肺炎是最常见的形式,SBP的发生率随ACLF分级增加而降低。COSSH-ACLF评分、急性肾损伤、BSI、凝血酶原活动度及侵入性导管插入术是28天结局的独立预测因素。