Akagi Tomonori, Inomata Masafumi, Hara Takao, Mizusawa Junki, Katayama Hiroshi, Shida Dai, Ohue Masayuki, Ito Masaaki, Kinugasa Yusuke, Saida Yoshihisa, Masaki Tadahiko, Yamamoto Seiichiro, Hanai Tsunekazu, Yamaguchi Shigeki, Watanabe Masahiko, Sugihara Kenichi, Fukuda Haruhiko, Kanemitsu Yukihide, Kitano Seigo
Gastroenterological and Pediatric Surgery Oita University of Faculty of Medicine Yufu Japan.
Japan Clinical Oncology Group Data Center/Operations Office National Cancer Center Hospital Tokyo Japan.
Ann Gastroenterol Surg. 2020 Feb 26;4(2):163-169. doi: 10.1002/ags3.12318. eCollection 2020 Mar.
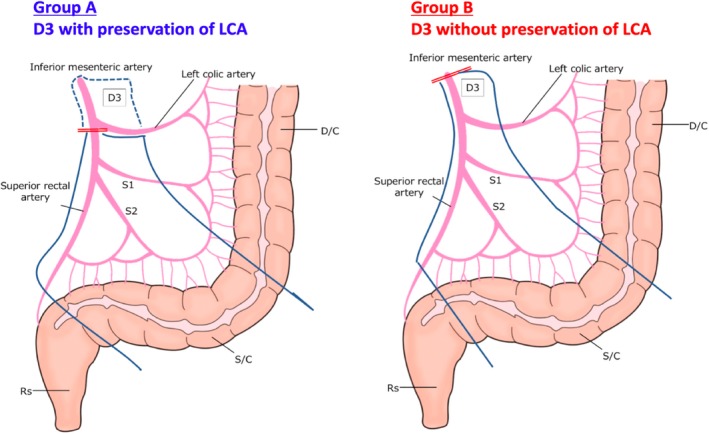
We investigated the clinical impact of D3 lymph node dissection preserving left colic artery (LCA) compared to D3 without LCA preservation using data from JCOG0404. LCA preservation is expected to maintain adequate blood supply, which is effective in preventing anastomotic leakage, intestinal paralysis, and bowel obstruction. Whether D3 with LCA preservation (Group A) improves clinical outcomes following resection of sigmoid colon cancer compared to D3 without LCA preservation (Group B) is unclear.
Procedure type was identified from photographs of the surgical field collected for central surgical review in JCOG0404. Clinical outcomes were compared between each procedure.
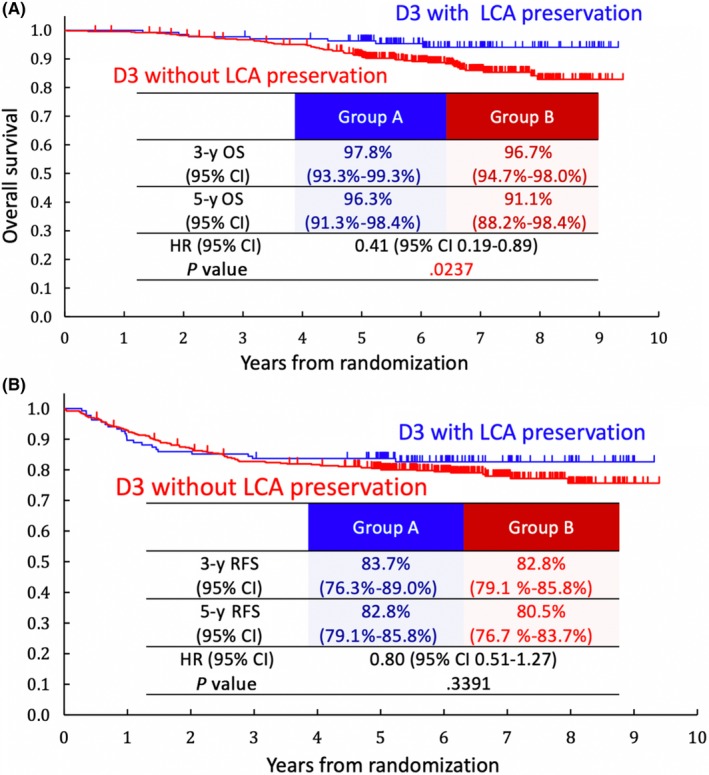
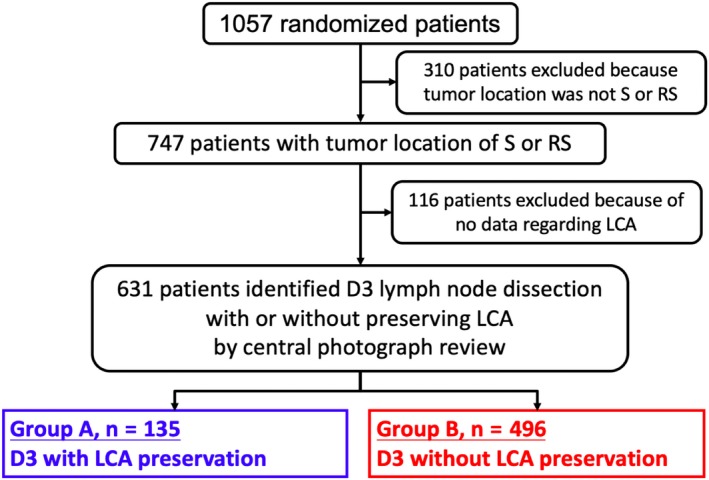
Among the 1057 randomized patients in JCOG0404, 631 patients receiving sigmoid colectomy or anterior resection were included in the subgroup analysis. Group A comprised of 135 patients and Group B of 496 patients. Patient backgrounds did not differ between groups. Median operative time, blood loss, anastomotic leakage, and intestinal paralysis were not remarkably different (Group A vs Group B: 185 vs 186 minutes, 60 vs 50 mL, 3.0% vs 5.0%, and 2.2% vs 3.8%). More overall postoperative complications occurred in Group B than Group A (21.6% vs 9.6%, = .022). Five-year relapse-free survival (RFS) and overall survival (OS) tended to be better in Group A than Group B (RFS: 83.7% and 80.5%, HR 0.80 [95% CI 0.51-1.26], OS: 96.3% and 91.1%, HR 0.41 [95% CI 0.19-0.89]).
Short- and long-term outcomes tend to be better in Group A than Group B, indicating that preservation of LCA could be an alternative treatment.
我们利用日本临床肿瘤学会(JCOG)0404的数据,研究了保留左结肠动脉(LCA)的D3淋巴结清扫术与未保留LCA的D3淋巴结清扫术相比的临床影响。保留LCA有望维持充足的血液供应,这对预防吻合口漏、肠麻痹和肠梗阻有效。与未保留LCA的D3(B组)相比,保留LCA的D3(A组)在乙状结肠癌切除术后是否能改善临床结局尚不清楚。
从JCOG0404中为中央手术评估收集的手术视野照片中确定手术类型。比较每种手术的临床结局。
在JCOG0404的1057例随机分组患者中,631例行乙状结肠切除术或前切除术的患者纳入亚组分析。A组135例患者,B组496例患者。两组患者背景无差异。中位手术时间、失血量、吻合口漏和肠麻痹无显著差异(A组 vs B组:185 vs 186分钟,60 vs 50 mL,3.0% vs 5.0%,2.2% vs 3.8%)。B组术后总体并发症比A组更多(21.6% vs 9.6%,P = 0.022)。A组的5年无复发生存率(RFS)和总生存率(OS)倾向于比B组更好(RFS:83.7%和80.5%,风险比0.80 [95%置信区间0.51 - 1.26],OS:96.3%和91.1%,风险比0.41 [95%置信区间0.19 - 0.89])。
A组的短期和长期结局倾向于比B组更好,表明保留LCA可能是一种替代治疗方法。