Department of General Surgery, Daping Hospital, Army Medical University, No. 10, Changjiang Branch Road, Daping, Yuzhong District, Chongqing, 400042, China.
BMC Surg. 2022 May 10;22(1):164. doi: 10.1186/s12893-022-01614-y.
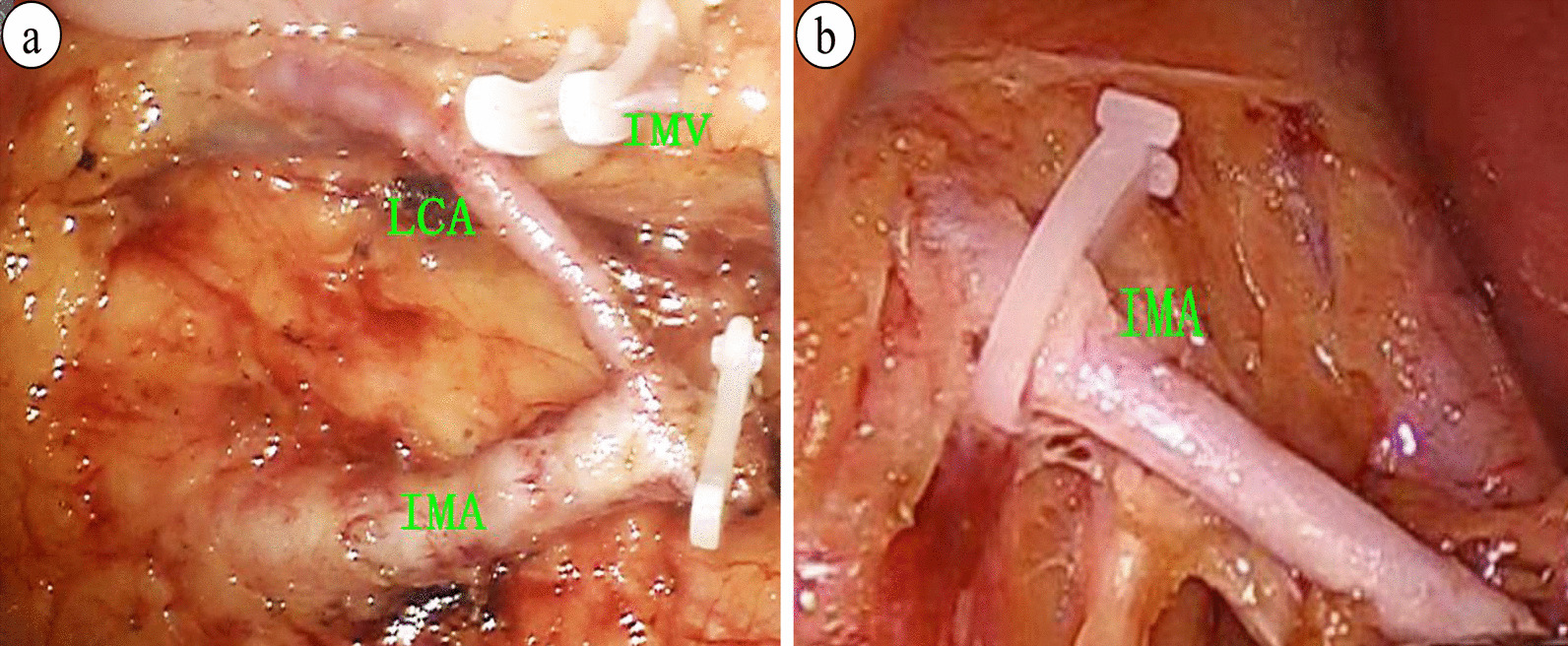
Preserving the left colic artery (LCA) during anterior resection for rectal cancer is controversial, and robust evidence of the outcomes of LCA preservation plus apical lymph node dissection is lacking. The purpose of this study was to investigate the impact of LCA preservation plus apical lymph node dissection surgery on anastomotic leakage and number of harvested lymph nodes.
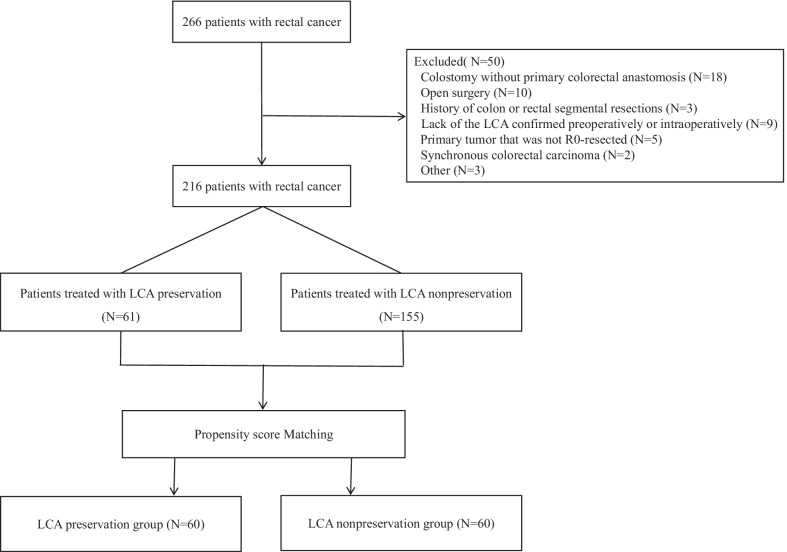
Patients who underwent laparoscopic or robotic anterior resection for rectal cancer between September 2017 and May 2020 were retrospectively assessed. The patients were categorized into two groups: preservation of LCA and nonpreservation of LCA. A one-to-one propensity score-matched analysis was performed to decrease confounding. The primary outcome was anastomotic leakage within 30 days after surgery. The secondary outcomes were number of harvested lymph nodes, 3-year overall survival, and 3-year disease-free survival.
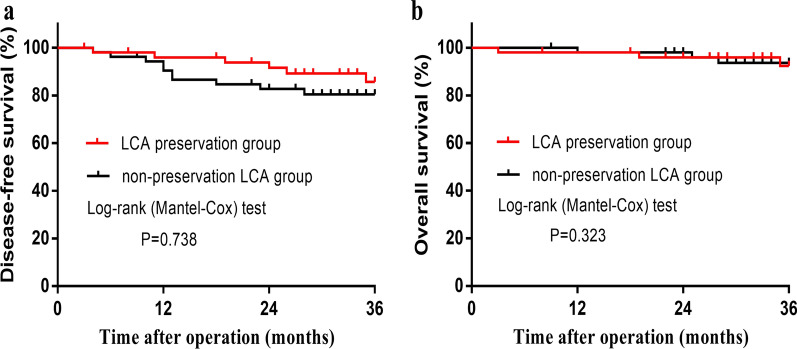
A total of 216 patients were eligible for this study, and propensity score matching yielded 60 patients in each group. Anastomotic leakage in the LCA preservation group was significantly lower than that in the LCA nonpreservation group (3.3% vs. 13.3%, P = 0.048). No significant differences were observed in blood loss, operation time, intraoperative complications, splenic flexure mobilization, total number of harvested lymph nodes, number of positive lymph nodes, time to first flatus, or postoperative hospital stay. Kaplan-Meier survival analysis showed a 3-year disease-free survival of 85.7% vs. 80.5% (P = 0.738) and overall survival of 92.4% vs. 93.7% (P = 0.323) for the preservation and nonpreservation groups, respectively.
LCA preservation plus apical lymph node dissection surgery for rectal cancer may help reduce the incidence of anastomotic leakage without impairing the number of harvested lymph nodes. Preliminary results suggest that 3-year disease-free survival and overall survival rates may not differ between the two types of surgery, but studies with larger sample sizes are needed to confirm these conclusions. Trial registration ClinicalTrials.gov, NCT03776370. Registered 14 December 2018-Retrospectively registered, https://clinicaltrials.gov .
在直肠癌前切除术时保留左结肠动脉(LCA)存在争议,缺乏关于 LCA 保留加顶端淋巴结清扫术结果的有力证据。本研究的目的是探讨 LCA 保留加顶端淋巴结清扫术对吻合口漏和淋巴结采集数量的影响。
回顾性评估 2017 年 9 月至 2020 年 5 月期间接受腹腔镜或机器人直肠癌前切除术的患者。将患者分为两组:保留 LCA 和不保留 LCA。进行 1:1 倾向评分匹配分析以减少混杂。主要结局为术后 30 天内吻合口漏。次要结局为采集的淋巴结数量、3 年总生存率和 3 年无病生存率。
共有 216 名患者符合本研究条件,倾向性评分匹配后每组各有 60 名患者。LCA 保留组的吻合口漏明显低于 LCA 不保留组(3.3%比 13.3%,P=0.048)。两组间出血量、手术时间、术中并发症、脾曲游离、采集的总淋巴结数量、阳性淋巴结数量、首次排气时间和术后住院时间均无显著差异。Kaplan-Meier 生存分析显示,保留组和不保留组的 3 年无病生存率分别为 85.7%和 80.5%(P=0.738),总生存率分别为 92.4%和 93.7%(P=0.323)。
直肠癌 LCA 保留加顶端淋巴结清扫术可能有助于降低吻合口漏的发生率,而不影响采集的淋巴结数量。初步结果表明,两种手术类型的 3 年无病生存率和总生存率可能没有差异,但需要更大样本量的研究来证实这些结论。
ClinicalTrials.gov,NCT03776370。于 2018 年 12 月 14 日注册-回顾性注册,https://clinicaltrials.gov。