Anesthesiology, Intensive Care and Pain Medicine, Universitatsklinikum Munster, Munster, Nordrhein-Westfalen, Germany.
Department of Critical Care, King's College London, Guy's & St Thomas' Hospital, London, UK.
BMJ Open. 2020 Apr 6;10(4):e034201. doi: 10.1136/bmjopen-2019-034201.
Acute kidney injury (AKI) is a frequent complication after cardiac surgery with adverse short-term and long-term outcomes. Although prevention of AKI (PrevAKI) is strongly recommended, the optimal strategy is uncertain. The Kidney Disease: Improving Global Outcomes (KDIGO) guideline recommended a bundle of supportive measures in high-risk patients. In a single-centre trial, we recently demonstrated that the strict implementation of the KDIGO bundle significantly reduced the occurrence of AKI after cardiac surgery. In this feasibility study, we aim to evaluate whether the study protocol can be implemented in a multicentre setting in preparation for a large multicentre trial.
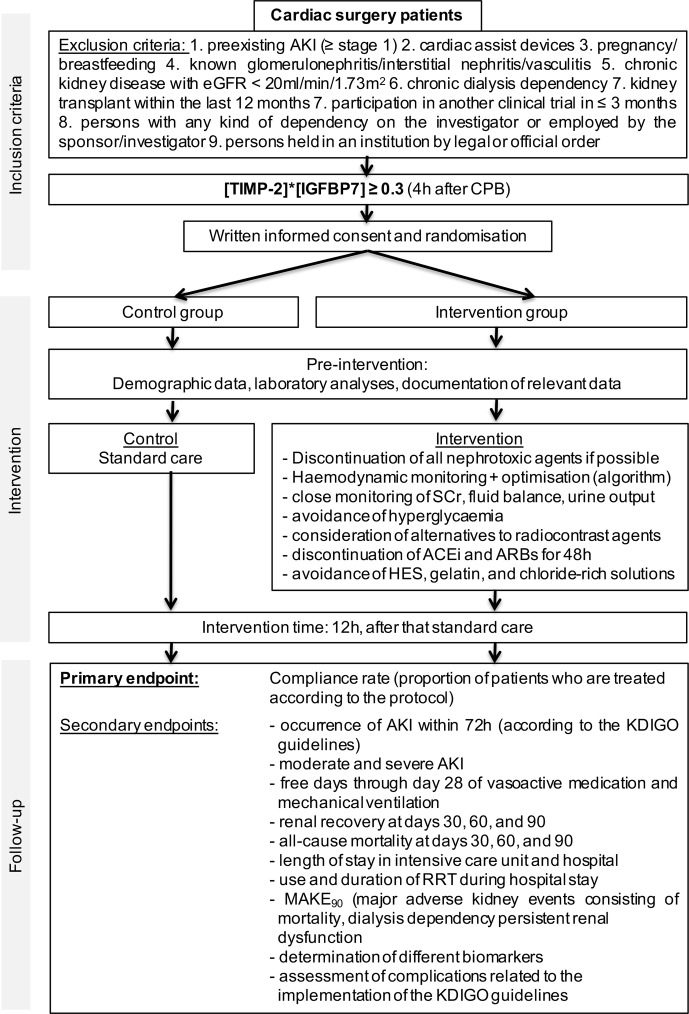
We plan to conduct a prospective, observational survey followed by a randomised controlled, multicentre, multinational clinical trial including 280 patients undergoing cardiac surgery with cardiopulmonary bypass. The purpose of the observational survey is to explore the adherence to the KDIGO recommendations in routine clinical practice. The second phase is a randomised controlled trial. The objective is to investigate whether the trial protocol is implementable in a large multicentre, multinational setting. The primary endpoint of the interventional part is the compliance rate with the protocol. Secondary endpoints include the occurrence of any AKI and moderate/severe AKI as defined by the KDIGO criteria within 72 hours after surgery, renal recovery at day 90, use of renal replacement therapy (RRT) and mortality at days 30, 60 and 90, the combined endpoint major adverse kidney events consisting of persistent renal dysfunction, RRT and mortality at day 90 and safety outcomes.
The PrevAKI multicentre study has been approved by the leading Research Ethics Committee of the University of Münster and the respective Research Ethics Committee at each participating site. The results will be used to design a large, definitive trial.
NCT03244514.
急性肾损伤(AKI)是心脏手术后常见的并发症,可导致短期和长期预后不良。尽管强烈推荐预防 AKI(PrevAKI),但最佳策略尚不确定。肾脏病:改善全球预后(KDIGO)指南建议高危患者采取一整套支持措施。在一项单中心试验中,我们最近证明,严格执行 KDIGO 指南可显著降低心脏手术后 AKI 的发生。在这项可行性研究中,我们旨在评估该研究方案是否可以在多中心环境中实施,为大型多中心试验做准备。
我们计划进行一项前瞻性、观察性调查,随后进行一项随机对照、多中心、多国临床试验,纳入 280 例行体外循环心脏手术的患者。观察性调查的目的是探讨常规临床实践中对 KDIGO 建议的依从性。第二阶段为随机对照试验。目的是研究该方案在大型多中心、多国家环境中的实施情况。干预部分的主要终点是方案的依从率。次要终点包括术后 72 小时内任何 AKI 和 KDIGO 标准定义的中重度 AKI 的发生、第 90 天的肾功能恢复、肾脏替代治疗(RRT)的使用以及第 30、60 和 90 天的死亡率、由持续性肾功能障碍、RRT 和第 90 天的死亡率组成的主要不良肾脏事件的复合终点以及安全性结局。
PrevAKI 多中心研究已获得明斯特大学主要研究伦理委员会和每个参与地点的相应研究伦理委员会的批准。研究结果将用于设计大型的、明确的试验。
NCT03244514。