Children's Hospital Oakland Research Institute, Oakland, CA, USA.
Department of Pediatrics, School of Medicine, University of California, San Francisco, CA, USA.
Am J Clin Nutr. 2020 Apr 1;111(4):927-937. doi: 10.1093/ajcn/nqz304.
The accurate estimation of zinc deficiency at the population level is important, as it guides the design, targeting, and evaluation of nutrition interventions. Plasma or serum zinc concentration (PZC) is recommended to estimate zinc nutritional status; however, concentrations may decrease in the presence of inflammation.
We aimed to assess the relation between PZC and inflammation in preschool children (PSC; 6-59 mo) and nonpregnant women of reproductive age (WRA; 15-49 y), and to compare different inflammation adjustment approaches, if adjustment is warranted.
Cross-sectional data from 13 nationally representative surveys (18,859 PSC, 22,695 WRA) from the Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) project were analyzed. Correlation and decile analyses were conducted, and the following 3 adjustment methods were compared if a consistent negative association between PZC and C-reactive protein (CRP) or α-1-acid glycoprotein (AGP) was observed: 1) exclude individuals with CRP > 5 mg/L or AGP > 1 g/L; 2) apply arithmetic correction factors; and 3) use the BRINDA regression correction (RC) approach.
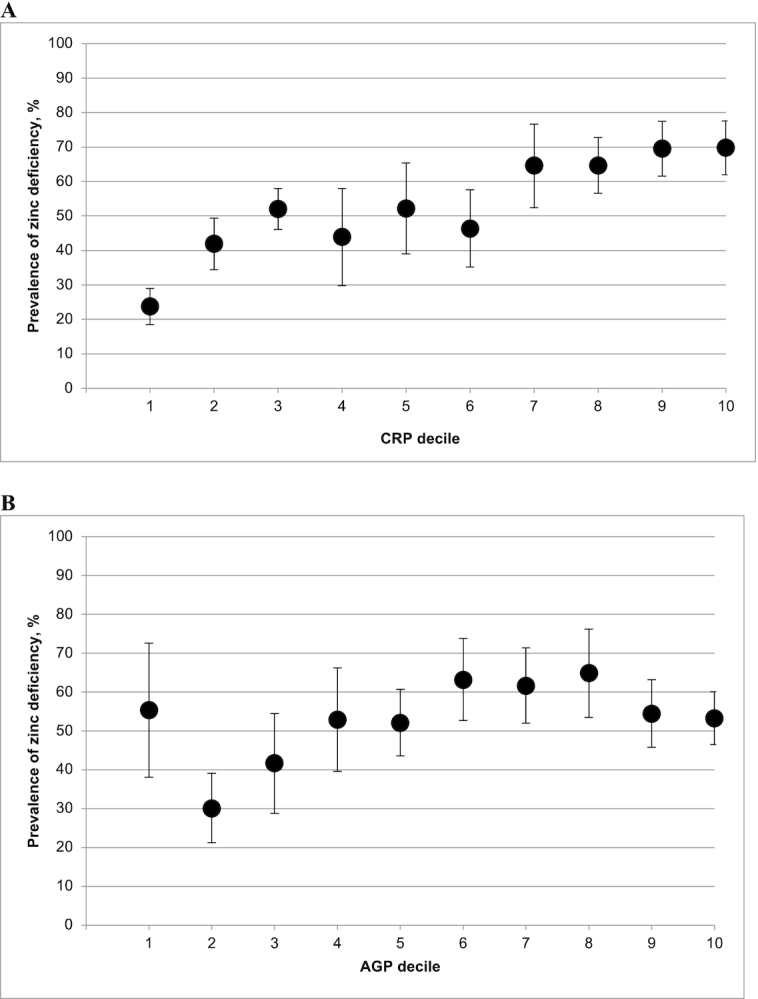
In 6 of 12 PSC surveys, the estimated prevalence of zinc deficiency increased with increasing CRP deciles, and to a lesser extent, with increasing AGP deciles. In WRA, the association of PZC with CRP and AGP was weak and inconsistent. In the 6 PSC surveys in which adjustment methods were compared, application of RC reduced the estimated prevalence of zinc deficiency by a median of 11 (range: 4-18) percentage points, compared with the unadjusted prevalence.
Relations between PZC and inflammatory markers were inconsistent, suggesting that correlation and decile analyses should be conducted before applying any inflammation adjustments. In populations of PSC that exhibit a significant negative association between PZC and CRP or AGP, application of the RC approach is supported. At this time, there is insufficient evidence to warrant inflammation adjustment in WRA.
准确评估人群的锌缺乏情况非常重要,因为它可以指导营养干预措施的设计、目标设定和评估。血浆或血清锌浓度(PZC)被推荐用于估计锌营养状况;然而,在存在炎症的情况下,浓度可能会降低。
我们旨在评估学龄前儿童(PSC;6-59 个月)和育龄妇女(WRA;15-49 岁)的 PZC 与炎症之间的关系,并在需要时比较不同的炎症调整方法。
对来自生物标志物反映炎症和营养决定贫血(BRINDA)项目的 13 项具有全国代表性的调查(18859 名 PSC,22695 名 WRA)的横断面数据进行了分析。进行了相关性和十分位数分析,如果观察到 PZC 与 C 反应蛋白(CRP)或α-1-酸性糖蛋白(AGP)之间存在一致的负相关,则比较了以下 3 种调整方法:1)排除 CRP>5mg/L 或 AGP>1g/L 的个体;2)应用算术校正因子;3)使用 BRINDA 回归校正(RC)方法。
在 12 项 PSC 调查中的 6 项中,随着 CRP 十分位数的增加,锌缺乏的估计患病率增加,而在 AGP 十分位数的增加则较少。在 WRA 中,PZC 与 CRP 和 AGP 的相关性较弱且不一致。在比较调整方法的 6 项 PSC 调查中,与未调整的患病率相比,RC 的应用中位数降低了锌缺乏的估计患病率 11(范围:4-18)个百分点。
PZC 与炎症标志物之间的关系不一致,这表明在应用任何炎症调整之前,应进行相关性和十分位数分析。在 PSC 人群中,如果观察到 PZC 与 CRP 或 AGP 之间存在显著的负相关,应应用 RC 方法。目前,没有足够的证据支持 WRA 的炎症调整。