School of Pharmacy, University of the Western Cape, Private Bag X17, Bellville, Cape Town, 7535, South Africa.
Neonatology Department, Netcare Blaauwberg Hospital, Sunningdale, Cape Town, 7441, South Africa.
Drugs R D. 2020 Jun;20(2):105-113. doi: 10.1007/s40268-020-00302-7.
The pharmacokinetics of vancomycin, a drug used for the treatment of methicillin-resistant Staphylococcus aureus (MRSA), varies between paediatric and adult patients.
The objective of this study was to assess the pharmacokinetics of vancomycin in preterm neonates and determine the optimum dose regimen.
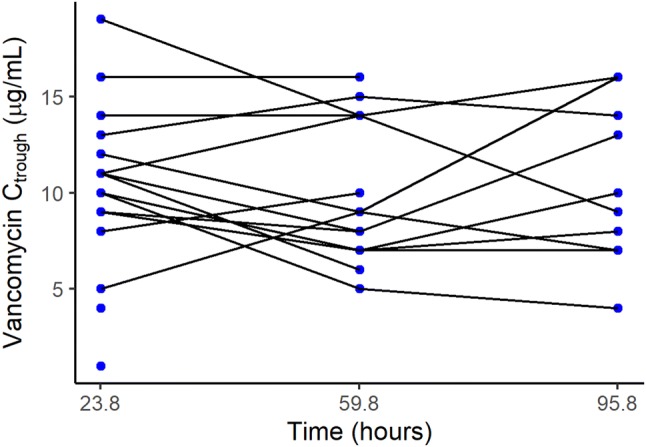
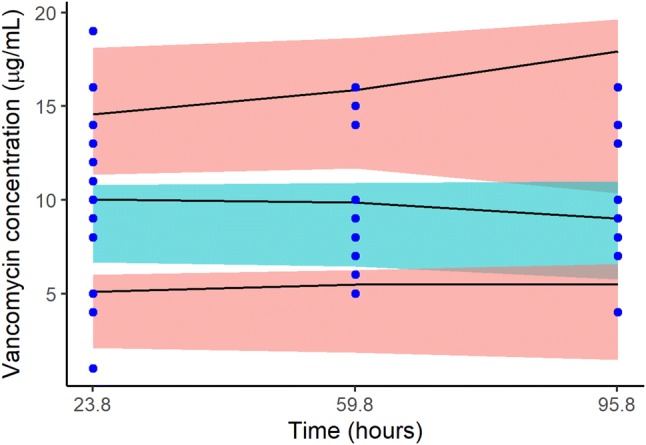
This was a randomised double-blind study of preterm neonates admitted to neonatal intensive care units. They all received vancomycin 15 mg/kg every 12 h. Blood was sampled just before administration of the third, sixth and ninth vancomycin dose. Pharmacokinetic parameters were estimated using a Bayesian approach implemented in Monolix 2018R2 software. Covariates assessed included postmenstrual age, current weight, creatinine clearance, albumin, gestational age, body surface area and current age. We used Monte Carlo simulations for dose regimen optimisation targeting area under the concentration-time curve up to 24 h (AUC) of ≥ 400 mg × h/L.
In total, 19 preterm neonates were enrolled in the study with a median age of 14 (3-58) days. A one-compartment model with linear elimination best described the pharmacokinetics of vancomycin. Volume of distribution and clearance was 0.88 L and 0.1 L/h, respectively, for a typical neonate weighing 1.48 kg. Simulation of the current dose regimen showed that 27.5% of the neonates would achieve the target AUC of ≥ 400 mg × h/L, and 70.7% of the neonates would achieve it with 12 mg/kg every 8 h.
The majority of the neonates were under dosed. Vancomycin 12 mg/kg should be administered every 8 h over 1 h infusion to improve the likelihood of achieving the AUC target of ≥ 400 mg × h/L. This target is considered optimal for MRSA infections, where the vancomycin minimum inhibitory concentration is ≤ 1 µg/mL.
万古霉素是一种用于治疗耐甲氧西林金黄色葡萄球菌(MRSA)的药物,其药代动力学在儿科和成人患者之间存在差异。
本研究旨在评估早产儿万古霉素的药代动力学,并确定最佳剂量方案。
这是一项纳入新生儿重症监护病房早产儿的随机双盲研究。他们均接受万古霉素 15mg/kg,每 12 小时一次。在万古霉素第 3、6 和 9 次给药前采集血样。采用贝叶斯方法在 Monolix 2018R2 软件中估算药代动力学参数。评估的协变量包括胎龄校正年龄、当前体重、肌酐清除率、白蛋白、胎龄、体表面积和当前年龄。我们使用蒙特卡罗模拟进行剂量方案优化,目标是达到 24 小时内浓度-时间曲线下面积(AUC)≥400mg·h/L。
共有 19 名胎龄 14(3-58)天的早产儿入组研究。万古霉素的药代动力学最好用单室模型加线性清除来描述。对于典型体重为 1.48kg 的新生儿,分布容积和清除率分别为 0.88L 和 0.1L/h。当前剂量方案的模拟结果显示,27.5%的新生儿将达到 AUC≥400mg·h/L 的目标,70.7%的新生儿将通过每 8 小时 12mg/kg 的剂量方案达到该目标。
大多数新生儿的剂量不足。万古霉素 12mg/kg 应每 8 小时静脉滴注 1 小时,以提高达到 AUC 目标≥400mg·h/L 的可能性。该目标被认为是治疗 MRSA 感染的最佳目标,此时万古霉素的最低抑菌浓度≤1μg/ml。