Maternal and Pediatric Infectious Disease Branch, Eunice Kennedy Shriver National Institute of Child Health and Human Development, Bethesda, MD.
Division of HIV/AIDS Prevention, Centers for Disease Control and Prevention, Atlanta, GA.
J Acquir Immune Defic Syndr. 2020 May 1;84(1):92-100. doi: 10.1097/QAI.0000000000002308.
Almost one-quarter of all new HIV diagnoses in the United States occur among persons aged 13-24 years. These youths have the poorest HIV care continuum (HCC) outcomes, yet few empirical youth-specific data are available.
The Strategic Multisite Initiative for the Identification, Linkage, and Engagement in Care of HIV-infected youth (SMILE) helped HIV-infected (mostly newly diagnosed) youth, aged 12-24 years, link to youth-friendly care, and evaluated each milestone of the HCC (October 2012-September 2014). Numbers of HIV-infected youth referred, linked, engaged, and retained in care were recorded, along with sociodemographics. Viral suppression (VS) was defined as ≥1 HIV viral load (VL) below the level of detection on study. Correlates of VS were examined using Cox proportional hazards models.
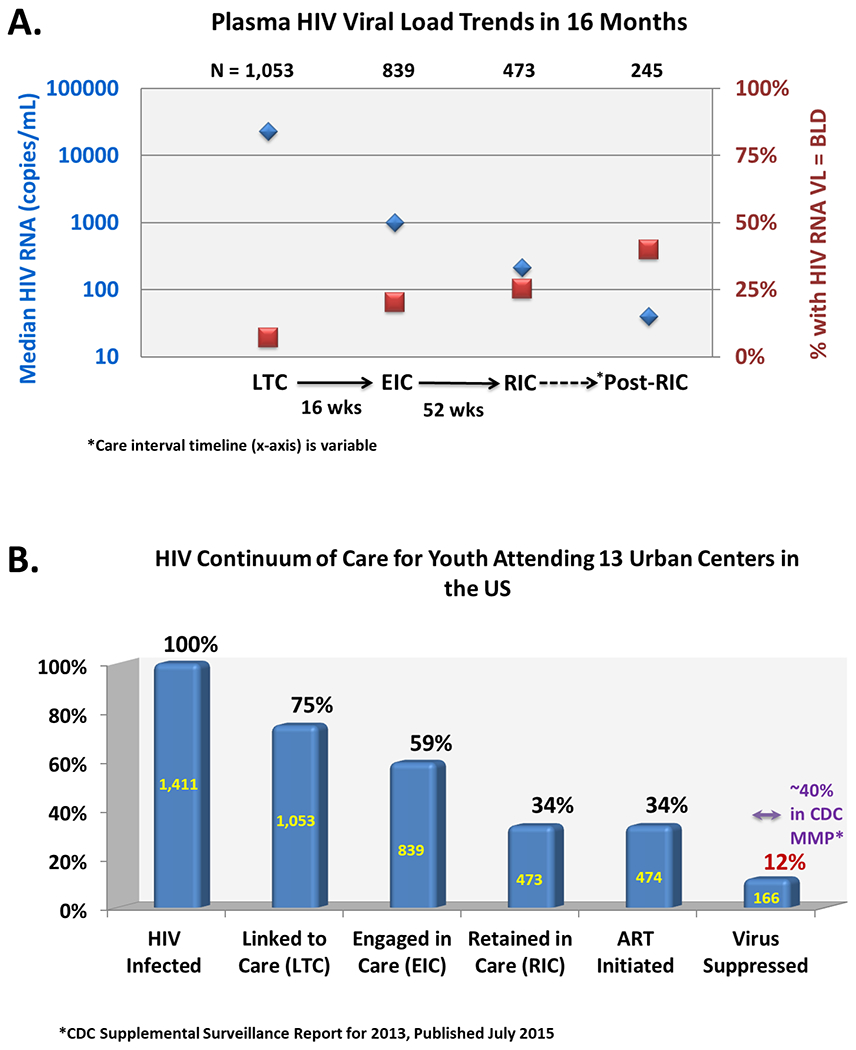
Among 1411 HIV-infected youth, 1053 (75%) were linked, 839 (59%) engaged, and 473 (34%) retained in care at adolescent health care sites. Antiretroviral therapy was initiated among 474 (34%), and 166 (12%) achieved VS. Predictors of VS included lower VL at baseline [aHR 1.56 (95% CI: 1.32-1.89), P < 0.0001], recent antiretroviral therapy receipt [aHR 3.10 (95% CI: 1.86-5.18), P < 0.0001], and shorter time from HIV testing until referral to linkage coordinator [aHR 2.52 (95% CI: 1.50-4.23), P = 0.0005 for 7 days to 6 weeks and aHR 2.08 (95% CI: 1.08-4.04), P = 0.0294 for 6 weeks to 3 months compared with >3 months].
Although this large national sample of predominately newly diagnosed youths linked to care at similar rates as adults, they achieved disproportionately lower rates of VS. Prompt referral to youth-friendly linkage services was an independent predictor of VS. Youth-focused interventions are urgently needed to improve their HCC outcomes.
美国近四分之一的新发 HIV 诊断发生在 13-24 岁的人群中。这些年轻人的 HIV 护理连续体(HCC)结局最差,但几乎没有针对年轻人的具体数据。
战略多地点倡议,以识别,联系和参与 HIV 感染的青年护理(SMILE)帮助 HIV 感染(主要是新诊断)的青年,年龄在 12-24 岁,联系到青年友好的护理,并评估 HCC 的每一个里程碑(2012 年 10 月至 2014 年 9 月)。记录了 HIV 感染的青年人数、联系人数、参与人数和保留在护理中的人数,以及社会人口统计学资料。病毒抑制(VS)的定义是在研究中低于检测水平的至少有一次 HIV 病毒载量(VL)。使用 Cox 比例风险模型检查 VS 的相关性。
在 1411 名 HIV 感染的青年中,有 1053 名(75%)在青少年保健机构中与 HIV 相关联,839 名(59%)参与,473 名(34%)保留在护理中。在 474 名(34%)中开始了抗逆转录病毒治疗,166 名(12%)达到了 VS。VS 的预测因素包括基线时较低的 VL [调整后的危险比 1.56(95%可信区间:1.32-1.89),P<0.0001]、最近接受抗逆转录病毒治疗[aHR 3.10(95%可信区间:1.86-5.18),P<0.0001]和从 HIV 检测到转介到联系协调员的时间较短[aHR 2.52(95%可信区间:1.50-4.23),P=0.0005,7 天至 6 周;aHR 2.08(95%可信区间:1.08-4.04),P=0.0294,6 周至 3 个月与 >3 个月相比]。
尽管这是一个大型的全国性新诊断青年样本,他们与成年人一样有相似的比例联系到护理,但他们的病毒抑制率却不成比例地低。及时转介到青年友好的联系服务是 VS 的一个独立预测因素。迫切需要以青年为中心的干预措施来改善他们的 HCC 结局。