Lundon Katie, Inrig Taucha, Paton Morag, Shupak Rachel, Kennedy Carol, McGlynn Mandy, Barber Claire
University of Toronto, Toronto, Ontario, Canada.
St. Michael's Hospital, Toronto, Ontario, Canada.
ACR Open Rheumatol. 2020 Apr;2(4):242-250. doi: 10.1002/acr2.11129. Epub 2020 Apr 11.
Our objective was to characterize Canadian workforce attributes of extended role practitioners (ERPs) in arthritis care.
We used an exploratory, mixed-methods study that was based on the Canadian Rheumatology Association's Stand Up and Be Counted Rheumatologist Workforce Survey (2015). An anonymous online survey was deployed to groups of non-physician health care professionals across Canada who potentially had post-licensure training in arthritis care. Demographic and practice information were elicited. Qualitative responses were analyzed using grounded theory techniques.
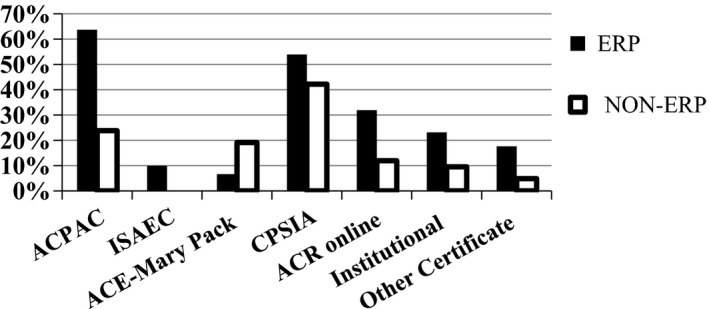
Of 141 respondents, 91 identified as practicing in extended role capacities. The mean age of ERP respondents was 48.7; 87% were female, and 41% of ERPs planned to retire within 5 to 10 years. Respondents were largely physical or occupational therapists by profession and practiced in urban/academic (46%), community (39%), and rural settings (13%). Differences in practice patterns were noted between ERPs (64.5%) and non-ERPs (34.5%), with more ERPs working in extended role capacities while retaining activities reflective of their professional backgrounds. Most respondents (95%) agreed that formal training is necessary to work as an ERP, but only half perceived they had sufficient training opportunities. Barriers to pursuing training were varied, including personal barriers, geographic barriers, patient-care needs, and financial/remuneration concerns.
To our knowledge, no previous studies have assessed the workforce capacity or the perceived need for the training of ERPs working in arthritis and musculoskeletal care. Measurement is important because in these health disciplines, practitioners' scopes of practice evolve, and ERPs integrate into the Canadian health care system. ERPs have emerged to augment provision of arthritis care, but funding for continuing professional development opportunities and for role implementation remains tenuous.
我们的目的是描述加拿大关节炎护理领域扩展职责从业者(ERP)的劳动力属性。
我们采用了一项探索性的混合方法研究,该研究基于加拿大风湿病协会的“站出来,被统计”风湿病医生劳动力调查(2015年)。向加拿大各地可能接受过关节炎护理执照后培训的非医生医疗保健专业人员群体开展了一项匿名在线调查。收集了人口统计学和实践信息。使用扎根理论技术对定性回答进行了分析。
在141名受访者中,91人确定以扩展职责的身份执业。ERP受访者的平均年龄为48.7岁;87%为女性,41%的ERP计划在5至10年内退休。受访者大多是物理治疗师或职业治疗师,在城市/学术环境(46%)、社区环境(39%)和农村环境(13%)中执业。ERP(64.5%)和非ERP(34.5%)之间的实践模式存在差异,更多的ERP以扩展职责的身份工作,同时保留反映其专业背景的活动。大多数受访者(95%)同意,作为一名ERP需要接受正规培训,但只有一半的人认为他们有足够的培训机会。追求培训的障碍多种多样,包括个人障碍、地理障碍、患者护理需求以及财务/薪酬问题。
据我们所知,以前没有研究评估过在关节炎和肌肉骨骼护理领域工作的ERP的劳动力能力或对培训的感知需求。测量很重要,因为在这些健康学科中,从业者的执业范围在不断演变,而且ERP融入了加拿大医疗保健系统。ERP的出现是为了增加关节炎护理的提供,但持续专业发展机会和角色实施的资金仍然不足。