Con Danny, Buckle Andrew, Nicoll Amanda J, Lubel John S
Department of Gastroenterology Eastern Health Melbourne Victoria Australia.
Eastern Health Clinical School Monash University Melbourne Victoria Australia.
JGH Open. 2019 Jul 18;4(2):106-112. doi: 10.1002/jgh3.12224. eCollection 2020 Apr.
Marked elevations of alanine aminotransferase (ALT) are caused by a limited number of underlying pathologies, including hepatic ischemia, drugs/toxins, viral hepatitis, and-rarely-autoimmune hepatitis. The aim of this study was to determine the relative incidence of pathologies resulting in ALT greater than 1000 IU/L and factors predicting clinical outcomes in an Australian cohort.
A retrospective cohort study of all adult patients with ALT levels greater than 1000 IU/L between January 2013 and December 2015 was conducted at a large teaching hospital network in Australia. Multivariable logistic regression analysis was used to determine predictors of etiology and mortality.
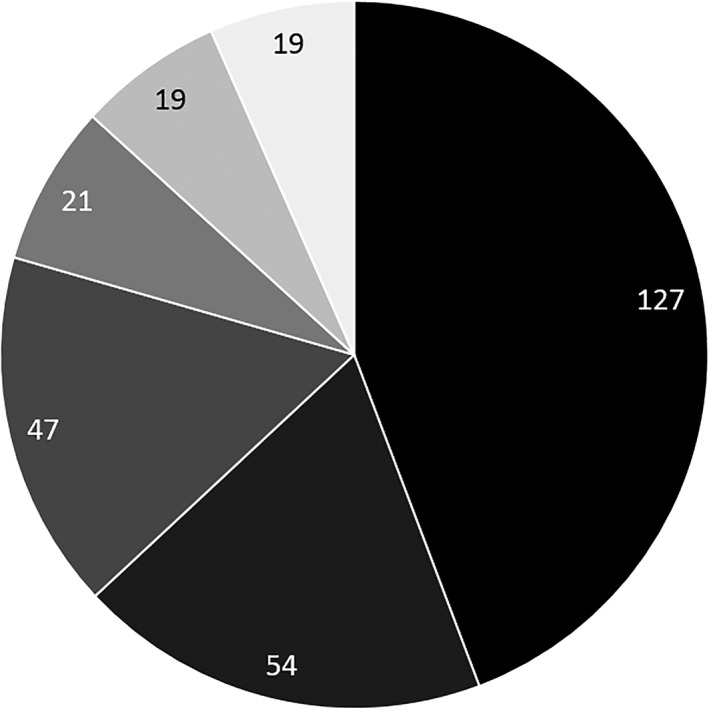
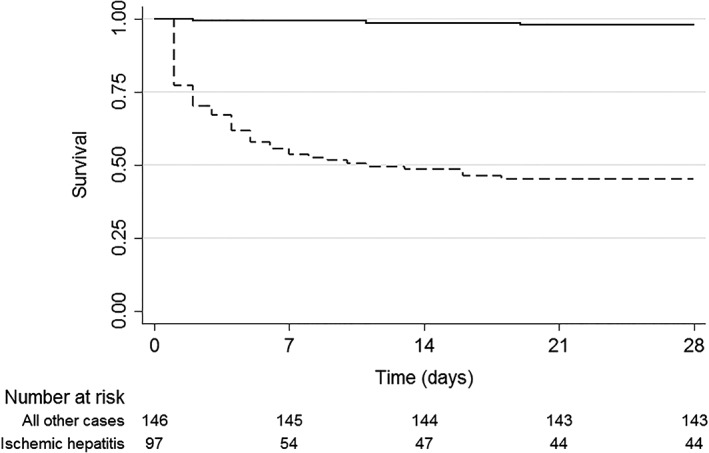
There were 287 patients identified with ALT levels greater than 1000 IU/L. The most common causes were ischemia (44%), drugs/toxins (19%), biliary obstruction (16%), and viral hepatitis (7%). Independent predictors of a diagnosis of ischemic hepatitis included (adjusted odds ratio; 95% confidence interval): hypotension (29.2; 8.2-104.7), chronic obstructive pulmonary disease (COPD) (20.2; 2.8-145.3), coronary artery disease (12.9; 1.7-98.9), congestive cardiac failure (7.8; 1.2-49.2), diabetes mellitus (7.4; 1.6-33.9), metabolic acidosis (6.2; 2.0-19.4), gamma-glutamyltransferase < 135 IU/L (5.1; 1.5-17.6), and albumin <34 g/L (3.4; 1.1-11.0). Independent risk factors for all-cause 28-day mortality included: septic shock (14.7; 4.3-50.7), metabolic acidosis (7.3; 2.5-21.3), history of COPD (5.4; 1.6-17.8), cardiogenic shock (4.3; 1.6-11.7), prothrombin time ≥ 20 s (3.7; 1.5-9.2), and age ≥ 65 years (3.0; 1.3-7.2).
Ischemic hepatitis was the most common cause of ALT levels greater than 1000 IU/L and was associated with high mortality.
丙氨酸氨基转移酶(ALT)显著升高是由少数潜在病变引起的,包括肝缺血、药物/毒素、病毒性肝炎,以及罕见的自身免疫性肝炎。本研究的目的是确定在澳大利亚队列中导致ALT大于1000 IU/L的病变的相对发病率以及预测临床结局的因素。
对2013年1月至2015年12月期间澳大利亚一家大型教学医院网络中所有ALT水平大于1000 IU/L的成年患者进行回顾性队列研究。采用多变量逻辑回归分析来确定病因和死亡率的预测因素。
共确定287例ALT水平大于1000 IU/L的患者。最常见的病因是缺血(44%)、药物/毒素(19%)、胆道梗阻(16%)和病毒性肝炎(7%)。缺血性肝炎诊断的独立预测因素包括(调整后的优势比;95%置信区间):低血压(29.2;8.2 - 104.7)、慢性阻塞性肺疾病(COPD)(20.2;2.8 - 145.3)、冠状动脉疾病(12.9;1.7 - 98.9)、充血性心力衰竭(7.8;1.2 - 49.2)、糖尿病(7.4;1.6 - 33.9)、代谢性酸中毒(6.2;2.0 - 19.4)、γ-谷氨酰转移酶<135 IU/L(5.1;1.5 - 17.6)和白蛋白<34 g/L(3.4;1.1 - 11.0)。全因28天死亡率的独立危险因素包括:感染性休克(14.7;4.3 - 50.7)、代谢性酸中毒(7.3;2.5 - 21.3)、COPD病史(5.4;1.6 - 17.8)、心源性休克(4.3;1.6 - 11.7)、凝血酶原时间≥20秒(3.7;1.5 - 9.2)和年龄≥65岁(3.0;1.3 - 7.2)。
缺血性肝炎是ALT水平大于1000 IU/L的最常见原因,且与高死亡率相关。