Division of Thoracic Oncology, Department of Thoracic Medicine, Chang Gung Memorial Hospital, Chang Gung University, College of Medicine, Taoyuan City, Taiwan.
Thoracic Oncology Unit, Chang Gung Memorial Hospital Cancer Center, Taoyuan City, Taiwan.
Thorac Cancer. 2020 Jun;11(6):1541-1549. doi: 10.1111/1759-7714.13426. Epub 2020 Apr 13.
Treatment for stage III non-small cell lung cancer (NSCLC) of unresectable disease mainly involves concurrent chemoradiation (CRT). Post-CRT consolidation treatment with durvalumab is a major therapeutic advance that provides survival benefit in this group of patients. However, the performance of this treatment strategy remains to be studied in a real-world setting.
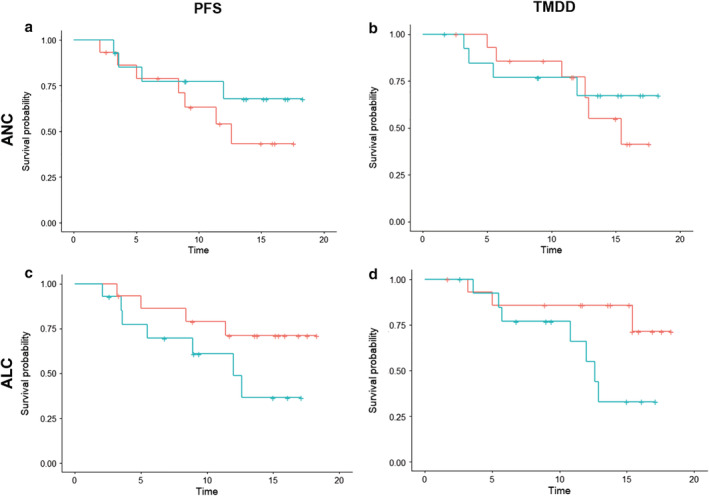
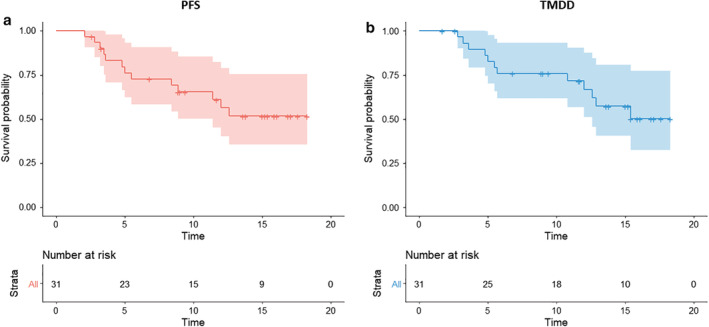
A total of 31 patients who had disease control post-CRT were included in the durvalumab early access program (EAP) as an intent-to-treat cohort and retrospectively reviewed for post-CRT progression-free survival (PFS) and time to metastatic disease or death (TMDD). The neutrophil-to-lymphocyte ratio (NLR) at the initiation of durvalumab was analyzed in 29 patients.
The median time from the completion of concurrent CRT to the initiation of durvalumb was 2.8 months. The objective response was 25.8% and the 12 month PFS and TMDD-free rate were 56.4% and 66.9%, respectively. The low NLR patients showed a significantly longer post-CRT PFS (not reach vs. 12.0 months [95% CI: 5.5-not estimable]; P = 0.040; the hazard ratio for disease progression or death, 0.23 [95% CI: 0.05-1.00]; P = 0.048) and the 12 month post-CRT PFS rate (82.5 vs. 42.6%). The post-CRT TMDD (not reach vs. 12.6 months, [95% CI: 10.8-not estimable]; P = 0.010; the hazard ratio for distant metastasis or death, 0.11 [95% CI: 0.01-0.88]; P = 0.037) and 12 month post-CRT TMDD-free rate (90.9 vs. 57.1%) were also significantly higher in the low NLR patients.
Durvalumab consolidation treatment in real-world patients showed substantial efficacy and the correlation with the NLR level warrants further investigation.
不可切除的 III 期非小细胞肺癌(NSCLC)的治疗主要涉及同期放化疗(CRT)。在 CRT 后进行度伐利尤单抗巩固治疗是一项重大治疗进展,为这组患者提供了生存获益。然而,这种治疗策略的疗效在真实环境中仍有待研究。
共有 31 例 CRT 后疾病得到控制的患者入组度伐利尤单抗早期准入计划(EAP)作为意向治疗队列,并对 CRT 后无进展生存期(PFS)和转移疾病或死亡时间(TMDD)进行回顾性分析。在 29 例患者中分析了起始度伐利尤单抗时的中性粒细胞与淋巴细胞比值(NLR)。
从同期 CRT 完成到开始度伐利尤单抗的中位时间为 2.8 个月。客观缓解率为 25.8%,12 个月 PFS 和 TMDD 无进展率分别为 56.4%和 66.9%。低 NLR 患者的 CRT 后 PFS 明显更长(未达到 vs. 12.0 个月[95%CI:5.5-不可估计];P = 0.040;疾病进展或死亡的风险比,0.23[95%CI:0.05-1.00];P = 0.048)和 12 个月 CRT 后 PFS 率(82.5% vs. 42.6%)。低 NLR 患者的 CRT 后 TMDD(未达到 vs. 12.6 个月[95%CI:10.8-不可估计];P = 0.010;远处转移或死亡的风险比,0.11[95%CI:0.01-0.88];P = 0.037)和 12 个月 CRT 后 TMDD 无进展率(90.9% vs. 57.1%)也显著更高。
真实世界中患者的度伐利尤单抗巩固治疗显示出显著的疗效,与 NLR 水平的相关性值得进一步研究。