Costache Mădălin Ionuţ, Cazacu Irina M, Dietrich Christoph F, Petrone Maria Chiara, Arcidiacono Paolo Giorgio, Giovannini Marc, Bories Erwan, Garcia Julio Iglesias, Siyu Sun, Santo Erwin, Popescu Carmen Florina, Constantin Alina, Bhutani Manoop S, Saftoiu Adrian
Research Center of Gastroenterology and Hepatology, University of Medicine and Pharmacy, Craiova, Romania.
Research Center of Gastroenterology and Hepatology, University of Medicine and Pharmacy, Craiova, Romania; Department of Gastroenterology, Hepatology and Nutrition, MD Anderson Cancer Center, Houston, Texas, USA.
Endosc Ultrasound. 2020 Mar-Apr;9(2):116-121. doi: 10.4103/eus.eus_69_19.
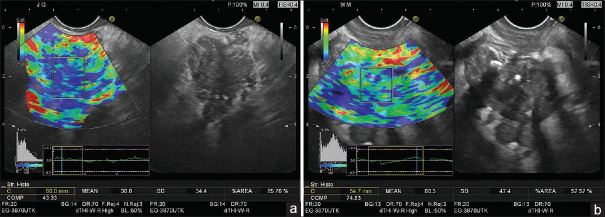
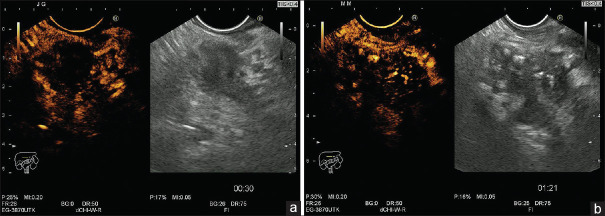
Recent advances in EUS techniques (real-time EUS elastography and contrast-enhanced EUS) have allowed a better characterization of focal pancreatic masses. Mean strain histograms (SHs) are considered a good parameter for the semi-quantitative evaluation of focal pancreatic masses, alongside complementary contrast-enhanced EUS parameters which can be quantified during both the early arterial and late venous phase.
The study design was prospective, blinded, and multicentric, assessing real-time EUS elastography and contrast-enhanced EUS results for the characterization of focal pancreatic masses using parametric measurements, in comparison with pathology which is the gold standard. SHs were performed based on the embedded software of the ultrasound system, with the values being reversed as opposed to our initially published data on hue histograms. Consequently, a cutoff of 80 was derived from previous multicentric trials. Contrast-enhanced EUS also allowed the focal masses to be classified as hyper-, iso-, or hypoenhanced in comparison with the normal pancreatic parenchyma. EUS-FNA was then performed for all patients, with a positive cytological diagnosis taken as a final proof of malignancy for the pancreatic masses. The diagnoses obtained by EUS-FNA were verified further either by surgery or during a clinical follow-up of at least 6 months.
A total number of 97 consecutive patients with focal pancreatic masses were included in the study. Based on previously defined cutoffs of 80, the values of sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of the mean SHs for the diagnosis of pancreatic cancer were 100%, 29.63%, 78.65%, 100%, and 80.41%, respectively. Corresponding values for contrast-enhanced EUS (taking into consideration hypoenhencement as a predictive factor of malignancy) were 98.57%, 77.78%, 92%, 95.45%, and 92.78%, respectively. Combining contrast enhancement-EUS (hypoenhencement) and semi-quantitative EUS elastography (SH cutoffs <80), the resulting values corresponding for sensitivity, specificity, and accuracy were 98.57%, 81.48%, and 93.81%, respectively.
The current study using objective parametric tools for both EUS elastography and contrast-enhanced EUS confirmed the results of previous studies and meta-analyses that indicated a complementary role for the differential diagnosis of focal pancreatic masses. Moreover, the best values for the receiver operating curves were obtained using a sequential clinical algorithm based on the initial use of elastography, followed by contrast enhancement.
超声内镜(EUS)技术(实时EUS弹性成像和对比增强EUS)的最新进展使胰腺局灶性肿块的特征得以更好地描述。平均应变直方图(SHs)被认为是胰腺局灶性肿块半定量评估的一个良好参数,同时还有可在动脉早期和静脉晚期进行量化的对比增强EUS补充参数。
本研究设计为前瞻性、盲法、多中心研究,通过参数测量评估实时EUS弹性成像和对比增强EUS结果以描述胰腺局灶性肿块特征,并与作为金标准的病理结果进行比较。SHs根据超声系统的嵌入式软件进行测量,与我们最初发表的关于色调直方图的数据相反,其值进行了反转。因此,根据之前的多中心试验得出截断值为80。对比增强EUS还可将局灶性肿块与正常胰腺实质相比分为高增强、等增强或低增强。然后对所有患者进行EUS-FNA,将阳性细胞学诊断作为胰腺肿块恶性肿瘤的最终确诊依据。通过手术或至少6个月的临床随访进一步验证EUS-FNA获得的诊断结果。
本研究共纳入97例连续的胰腺局灶性肿块患者。根据之前定义的截断值80,平均SHs诊断胰腺癌的敏感性、特异性、阳性预测值、阴性预测值和准确性分别为100%、29.63%、78.65%、100%和80.41%。对比增强EUS(将低增强作为恶性肿瘤的预测因素)的相应值分别为98.57%、77.78%、92%、95.45%和92.78%。将对比增强EUS(低增强)和半定量EUS弹性成像(SH截断值<80)相结合,敏感性、特异性和准确性的相应值分别为98.57%、81.48%和93.81%。
本研究使用针对EUS弹性成像和对比增强EUS的客观参数工具,证实了之前研究和荟萃分析的结果,即两者在胰腺局灶性肿块的鉴别诊断中具有互补作用。此外,基于最初使用弹性成像,随后进行对比增强的序贯临床算法获得了最佳的受试者工作曲线值。