Singh J, Dhillon M S, Dhatt S S
Department of Orthopaedics, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India.
Department of Orthopaedics, Post Graduate Institute of Medical Education and Research, Chandigarh, India.
Malays Orthop J. 2020 Mar;14(1):61-73. doi: 10.5704/MOJ.2003.010.
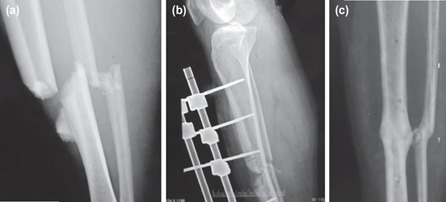
Grade 3B/C open tibial fractures with grossly contaminated degloving injuries have poor outcomes, with or without vascular injuries. Treatment decision oscillates between limb salvage and amputation. The standard protocol of repeated debridement and delayed wound cover is a challenge in developing countries due to overcrowded emergencies and limited operating room availability. We present results of our modified protocol involving primary stabilisation with external fixation and immediate wound cover as an aggressive modality of treatment.
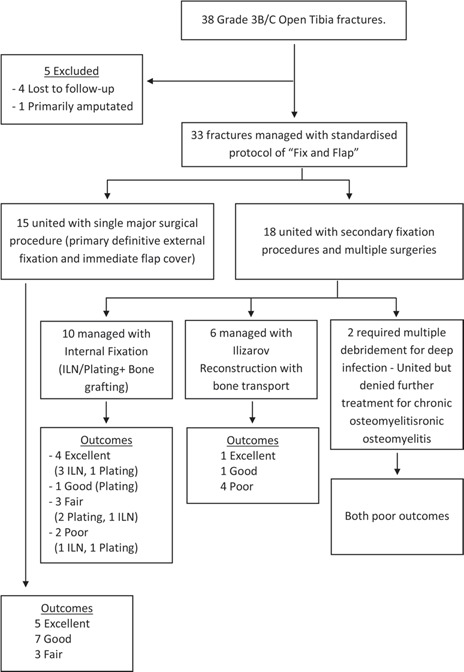
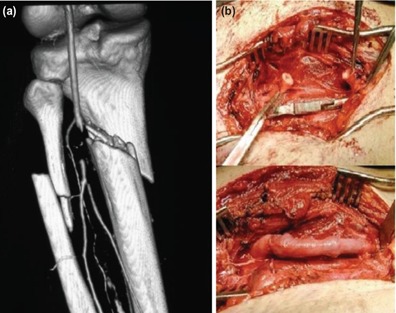
Thirty-three patients with severe open tibial shaft fractures were managed using a standardised protocol of emergent debridement, external fixation and immediate wound cover with free distant/local rotational muscle flaps and fasciocutaneous flaps, and with vascular repair in Grade 3C fractures. Intra-articular fractures were excluded. Patients were followed for a minimum of three years, with an assessment of clinical, radiological and functional outcomes.
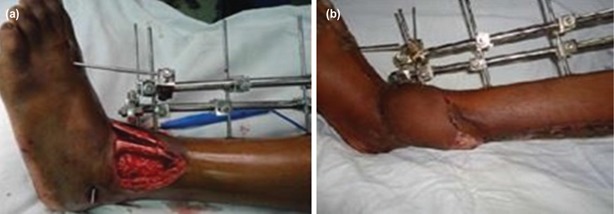
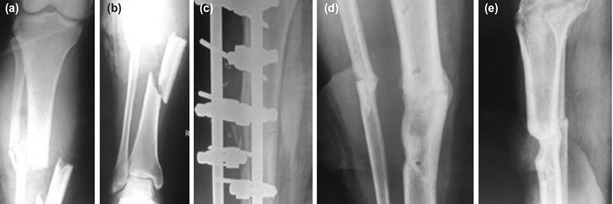
Wound cover was achieved with 24 distant free muscle flaps, four local rotational muscle flaps and five fasciocutaneous flaps. All fractures united with an average time to union of 40.3 weeks (16-88). Fifteen patients (45.4%) underwent only a single major surgery using primary definitive external fixation. Deep infection was seen in four patients (12.1%). Nineteen patients had excellent to good outcomes, six were fair, and eight were poor.
"Fix and Flap" in the same sitting, using immediate wound cover and external fixation, has given good results in our hands despite the delayed presentation, the neurovascular deficit and the degloving injury. This may be a better management strategy in overcrowded tertiary care centres of developing countries, with a single surgical procedure in almost half the cases.
伴有严重污染的脱套伤的3B/C级开放性胫骨骨折,无论有无血管损伤,预后均较差。治疗决策在保肢和截肢之间摇摆不定。由于急诊患者过多且手术室资源有限,在发展中国家,重复清创和延迟伤口覆盖的标准方案是一项挑战。我们展示了我们改良方案的结果,该方案包括使用外固定进行一期稳定以及立即进行伤口覆盖,作为一种积极的治疗方式。
33例严重开放性胫骨干骨折患者采用标准化方案进行治疗,包括急诊清创、外固定以及立即使用游离远位/局部旋转肌皮瓣和筋膜皮瓣进行伤口覆盖,对于3C级骨折进行血管修复。排除关节内骨折。对患者进行至少三年的随访,评估临床、影像学和功能结果。
使用24块游离远位肌皮瓣、4块局部旋转肌皮瓣和5块筋膜皮瓣实现了伤口覆盖。所有骨折均愈合,平均愈合时间为40.3周(16 - 88周)。15例患者(45.4%)仅接受了一次使用一期确定性外固定的大手术。4例患者(12.1%)发生深部感染。19例患者预后为优至良,6例为中等,8例为差。
在同一手术中进行“固定和皮瓣覆盖”,即立即进行伤口覆盖和外固定,尽管存在就诊延迟、神经血管缺损和脱套伤等情况,但在我们手中取得了良好的效果。对于发展中国家拥挤的三级医疗中心而言,这可能是一种更好的管理策略,几乎一半的病例只需进行一次外科手术。