Munthali Tendai, Michelo Charles, Mee Paul, Todd Jim
School of Public Health, University of Zambia, Lusaka, Zambia.
Department of Public Health, Ministry of Health, Lusaka, Zambia.
Front Public Health. 2020 Mar 31;8:96. doi: 10.3389/fpubh.2020.00096. eCollection 2020.
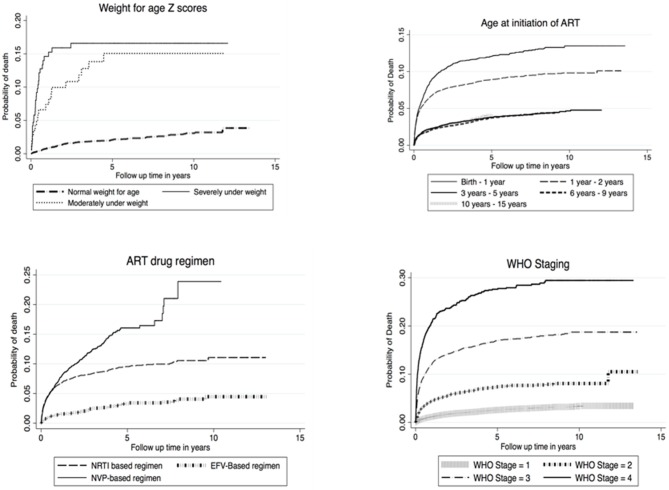
Research conducted before the introduction of anti-retroviral therapy (ART), showed that the majority of children living with HIV (CLHIV) would die before their second birthday. In Zambia, ART was rolled out to the public health system in 2004 with subsequent improved survival in CLHIV. However, the survival rates of CLHIV on ART in Zambia since 2004 have not been extensively documented. We assessed survival experiences and the factors associated with survival in CLHIV on ART in Zambia. We conducted a retrospective cohort analysis of CLHIV (aged up to 15 years) using routinely collected data from health facilities across Zambia, over 13 years to ascertain mortality rates. We explored survival factors using Cox regression giving adjusted hazard ratios (AHR) and 95% confidence intervals (95% CI). Nelson Aalen estimates were used to show the cumulative hazards of mortality for different levels of explanatory factors. A total of 65,448 eligible children, were initiated on ART between 2005 and 2018, of which 33,483 (51%) where female. They contributed a total survival time of 275,715-person years at risk during which 3,265 children died which translated into an incidence rate of 1.1 deaths per 100 person-years during the review period. Mortality rates were highest in children in the first year of life (Mortality rate 2.24; 95% CI = 2.08-2.42) and during the first year on ART (Mortality rate 3.82 95% CI = 3.67-3.98). Over 50% of the children had been on ART for 5-10 years by 2018, and they had the lowest risk of mortality compared to children who had been on ART for <5 years. Children with HIV in Zambia are surviving much longer than was predicted before ART was introduced 14 years ago. This key finding adds to the literature on analysis of survival in CLHIV in low income settings like Zambia. However, this survival is dependent on the age at which ART is initiated and the time on ART highlighting the need to increase investments in early infant diagnosis (EID) to ensure timely HIV testing and ART initiation for CLHIV.
在抗逆转录病毒疗法(ART)引入之前进行的研究表明,大多数感染艾滋病毒的儿童(CLHIV)会在两岁生日前死亡。在赞比亚,2004年抗逆转录病毒疗法被推广到公共卫生系统,随后感染艾滋病毒的儿童的存活率有所提高。然而,自2004年以来,赞比亚接受抗逆转录病毒疗法的感染艾滋病毒儿童的存活率尚未得到广泛记录。我们评估了赞比亚接受抗逆转录病毒疗法的感染艾滋病毒儿童的生存经历以及与生存相关的因素。我们使用从赞比亚各地医疗机构常规收集的数据,对13年间年龄在15岁及以下的感染艾滋病毒儿童进行了回顾性队列分析,以确定死亡率。我们使用Cox回归探索生存因素,给出调整后的风险比(AHR)和95%置信区间(95%CI)。Nelson Aalen估计值用于显示不同水平解释因素的累积死亡风险。2005年至2018年期间,共有65448名符合条件的儿童开始接受抗逆转录病毒疗法,其中33483名(51%)为女性。他们总共贡献了275715人年的风险生存时间,在此期间有3265名儿童死亡,这意味着在审查期间发病率为每100人年1.1例死亡。死亡率在出生后第一年的儿童中最高(死亡率2.24;95%CI = 2.08 - 2.42),以及在开始接受抗逆转录病毒疗法的第一年(死亡率3.82,95%CI = 3.67 - 3.98)。到2018年,超过50%的儿童接受抗逆转录病毒疗法已达5至10年,与接受抗逆转录病毒疗法不到5年的儿童相比,他们的死亡风险最低。赞比亚感染艾滋病毒的儿童的存活时间比14年前引入抗逆转录病毒疗法之前预测的要长得多。这一关键发现丰富了关于赞比亚等低收入环境中感染艾滋病毒儿童生存分析的文献。然而,这种生存取决于开始接受抗逆转录病毒疗法的年龄以及接受治疗的时间,这突出表明需要增加对早期婴儿诊断(EID)的投资,以确保为感染艾滋病毒的儿童及时进行艾滋病毒检测和开始接受抗逆转录病毒疗法。