Ebonyi Augustine O, Oguche Stephen, Meloni Seema T, Sagay Solomon A, Kyriacou Demetrios N, Achenbach Chad J, Agbaji Oche O, Oyebode Tinuade A, Okonkwo Prosper, Idoko John A, Kanki Phyllis J
Department of Paediatrics, University of Jos/ Jos University Teaching Hospital, Jos, Nigeria.
Department of Immunology and Infectious Diseases, Harvard School of Public Health, Boston, MA, USA.
J AIDS Clin Res. 2014;5(12). doi: 10.4172/2155-6113.1000403. Epub 2014 Dec 20.
Mortality among human immunodeficiency virus-1 (HIV-1) infected children initiated on antiretroviral therapy (ART) though on a decline still remains high in resource-limited countries (RLC). Identifying baseline factors that predict mortality could allow their possible modification in order to improve pediatric HIV care and reduce mortality.
We conducted a retrospective cohort study analyzing data on 691 children, aged 2 months-15 years, diagnosed with HIV-1 infection and initiated on ART between July 2005 and March 2013 at the pediatric HIV clinic of Jos University Teaching Hospital. Lost to follow-up children were excluded from the analyses. A multivariate Cox proportional hazards model was fitted to identify predictors of mortality.
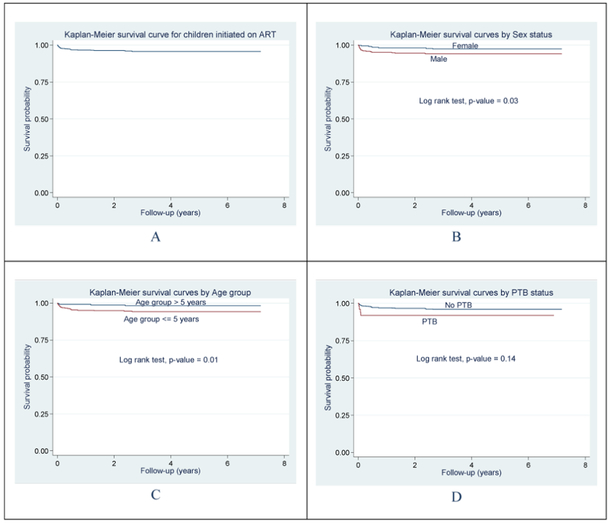
Median follow-up time for the 691 children initiated on ART was 4.4 years (interquartile range (IQR), 1.8-5.9) and at the end of 2752 person-years of follow-up, 32 (4.6%) had died and 659 (95.4%) survived. The mortality rate was 1.0 per 100 child-years of follow-up period. The median age of those who died was about two times lower than that of survivors [1.7 years (IQR, 0.6-3.6) versus 3.9 years (IQR, 3.9-10.3), p<0.001]. On unadjusted Cox regression, the risk of dying was about three and half times more in children <5 years of age compared to those >5 years (p=0.02) Multivariate modeling identified age as the main predictor of death with mortality decreasing by 24% for every 1 year increase in age (Adjusted Hazard Ratio (AHR)=0.76 [0.62-0.94], p=0.013.
The lower mortality rate for our study suggests that even in RLC, mortality rates could be reduced given a good standard of care. Early initiation of ART in younger children with close monitoring during follow-up could further reduce mortality.
在资源有限的国家(RLC),接受抗逆转录病毒治疗(ART)的人类免疫缺陷病毒1型(HIV-1)感染儿童的死亡率虽呈下降趋势,但仍然很高。确定预测死亡率的基线因素可以对其进行可能的调整,以改善儿科HIV护理并降低死亡率。
我们进行了一项回顾性队列研究,分析了2005年7月至2013年3月期间在乔斯大学教学医院儿科HIV诊所诊断为HIV-1感染并开始接受ART治疗的691名2个月至15岁儿童的数据。失访儿童被排除在分析之外。采用多变量Cox比例风险模型来确定死亡率的预测因素。
691名开始接受ART治疗的儿童的中位随访时间为4.4年(四分位间距(IQR),1.8 - 5.9),在2752人年的随访结束时,32名(4.6%)儿童死亡,659名(95.4%)存活。随访期内的死亡率为每100儿童年1.0例。死亡儿童的中位年龄比存活儿童低约两倍[1.7岁(IQR,0.6 - 3.6)对3.9岁(IQR,3.9 - 10.3),p<0.001]。在未经调整的Cox回归分析中,5岁以下儿童的死亡风险比5岁以上儿童高约3.5倍(p = 0.02)。多变量建模确定年龄是死亡的主要预测因素,年龄每增加1岁,死亡率降低24%(调整后风险比(AHR)=0.76 [0.62 - 0.94],p = 0.013)。
我们研究中较低的死亡率表明,即使在资源有限的国家,给予良好的护理标准也可以降低死亡率。对年幼儿童尽早开始ART治疗并在随访期间密切监测可以进一步降低死亡率。