Arlegui Hugo, Nachbaur Gaëlle, Praet Nicolas, Bégaud Bernard
INSERM, Bordeaux Population Health Research Center, Team Pharmacoepidemiology, UMR 1219, University of Bordeaux, Bordeaux, France.
Pharmaco-Epidemiology and Health Outcomes Research, GSK, Rueil-Malmaison, France.
Open Forum Infect Dis. 2020 Mar 12;7(4):ofaa087. doi: 10.1093/ofid/ofaa087. eCollection 2020 Apr.
Although rotavirus vaccines have proven to prevent the risk of rotavirus gastroenteritis (RVGE) in children under 5 years old, they are also associated with an increased transient risk of intussusception (IS). Several quantitative benefit-risk models (qBRm) are performed to measure this balance in hospitalizations and deaths prevented versus the ones induced.
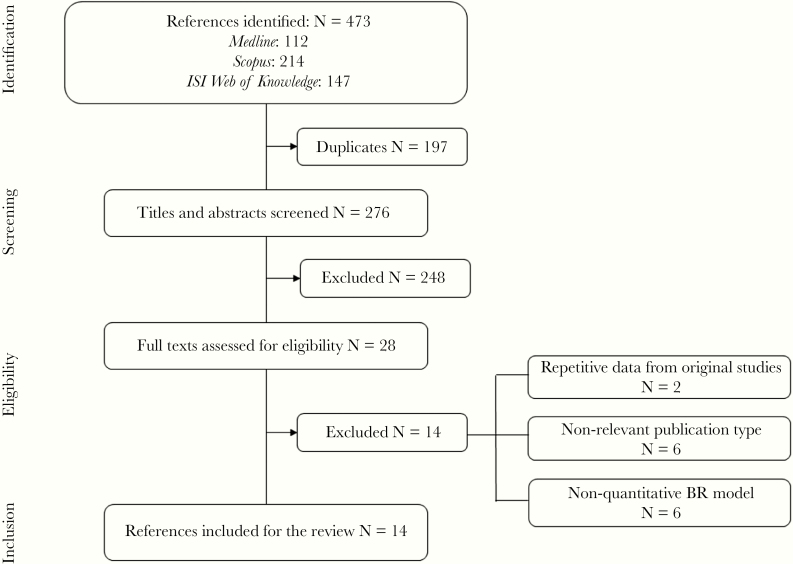
In this study, our objective was to provide a complete overview of qBRm used for rotavirus vaccination. We systematically searched 3 medical literature databases to identify relevant articles, in English, that were published between 2006 and 2019.
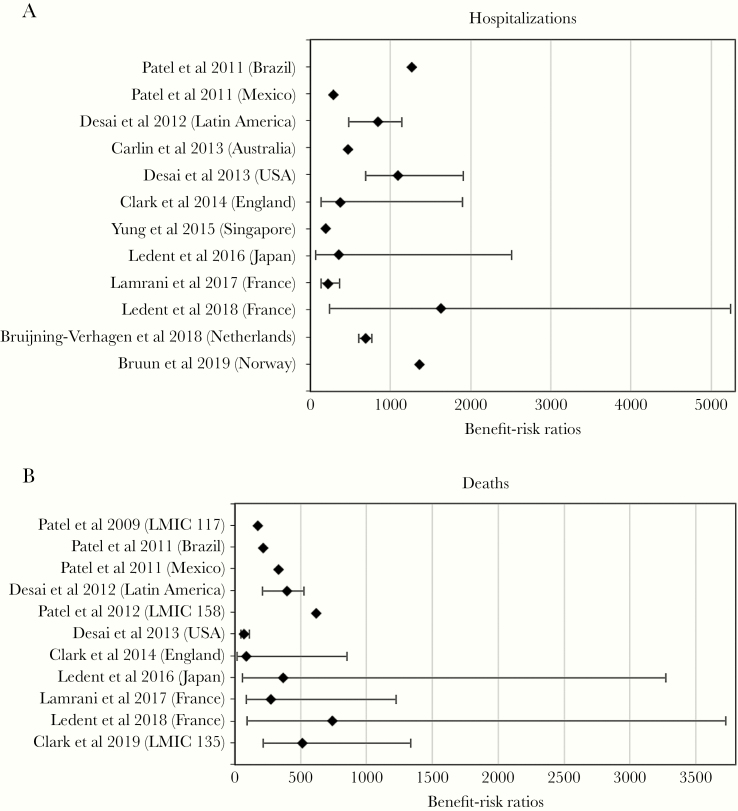
Of the 276 publications screened, 14 studies using qBRm for rotavirus vaccination were retained, based on preselected criteria. Four were performed in low- and middle-income countries. Almost all (13 of 14) displayed the following characteristics: force of infection assumed to be constant over time (static model), indirect effect of rotavirus vaccination (herd effect) not considered, closed model (individuals not allowed to enter and/or exit the model over time), and aggregated level (no tracking of individual's behavior). Most of the models were probabilistic (9 of 14) and reported sensitivity and/or scenario analyses (12 of 14). Input parameter values varied across studies. Selected studies suggest that, depending on the models used, for every IS hospitalization and death induced, vaccination would prevent, respectively, 190-1624 and 71-743 RVGE-related hospitalizations and deaths.
The benefits of rotavirus vaccination were shown to largely exceed the increased risk of IS, across all studies. Future research aiming to harmonize qBRm for rotavirus vaccination should ensure the comparability of studies and provide additional information for regulatory authorities, physicians, and patients.
尽管轮状病毒疫苗已被证明可预防5岁以下儿童患轮状病毒肠胃炎(RVGE)的风险,但它们也与肠套叠(IS)的短暂风险增加有关。已开展了几种定量效益风险模型(qBRm)来衡量这种平衡,即预防的住院和死亡病例与引发的住院和死亡病例之间的平衡。
在本研究中,我们的目标是全面概述用于轮状病毒疫苗接种的qBRm。我们系统检索了3个医学文献数据库,以识别2006年至2019年期间发表的相关英文文章。
在筛选的276篇出版物中,根据预先选定的标准,保留了14项使用qBRm进行轮状病毒疫苗接种的研究。其中4项在低收入和中等收入国家开展。几乎所有研究(14项中的13项)都具有以下特征:假设感染强度随时间恒定(静态模型),未考虑轮状病毒疫苗接种的间接效应(群体效应),封闭模型(个体不允许随时间进入和/或退出模型),以及总体水平(不跟踪个体行为)。大多数模型是概率性的(14项中的9项),并报告了敏感性和/或情景分析(14项中的12项)。不同研究的输入参数值各不相同。选定的研究表明,根据所使用的模型不同,每引发1例IS住院和死亡病例,疫苗接种分别可预防190 - 1624例和71 - 743例与RVGE相关的住院和死亡病例。
在所有研究中,轮状病毒疫苗接种的益处被证明在很大程度上超过了IS风险的增加。未来旨在统一用于轮状病毒疫苗接种的qBRm的研究应确保研究的可比性,并为监管机构、医生和患者提供更多信息。