Division of Cardiology, Department of Internal Medicine, University of Texas Southwestern Medical Center, Dallas (N.S.H., M.H.D.).
Winters Center for Heart Failure Research, Cardiovascular Research Institute, Baylor College of Medicine, Michael E. DeBakey VA Medical Center, Houston, TX (B.B.).
Circulation. 2020 Jun 9;141(23):1903-1914. doi: 10.1161/CIRCULATIONAHA.120.047349. Epub 2020 Apr 16.
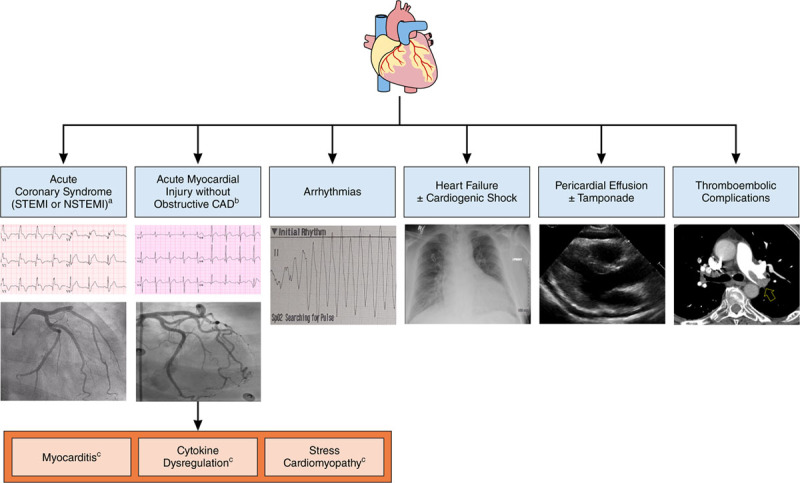
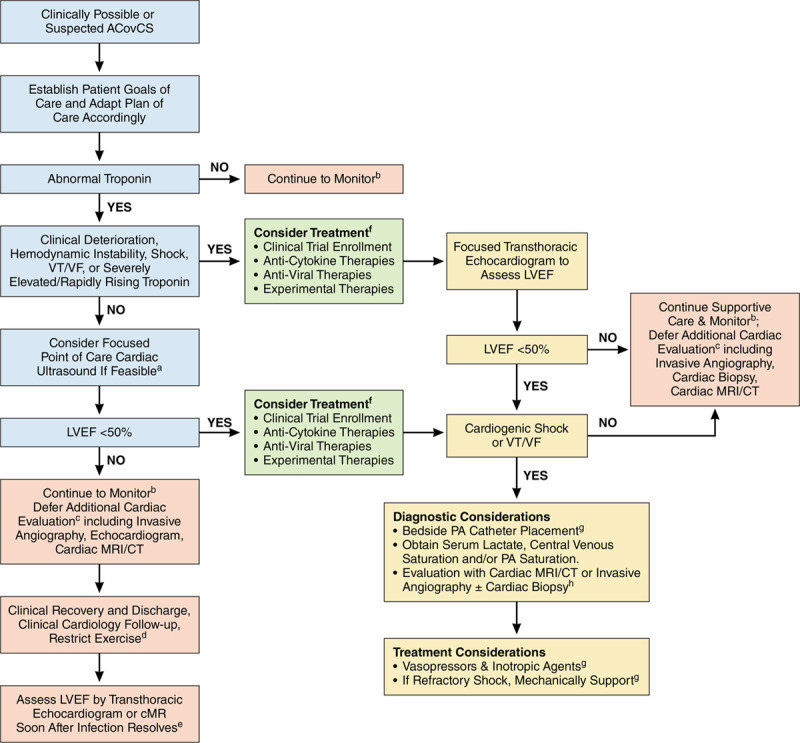
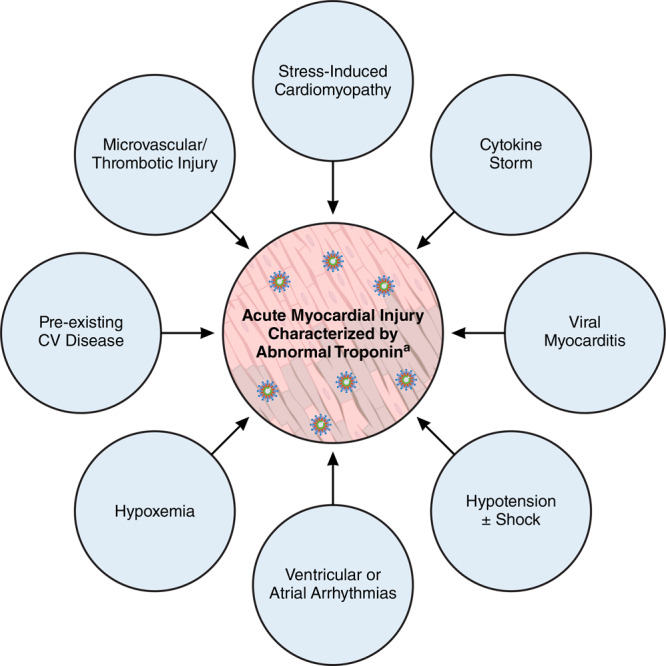
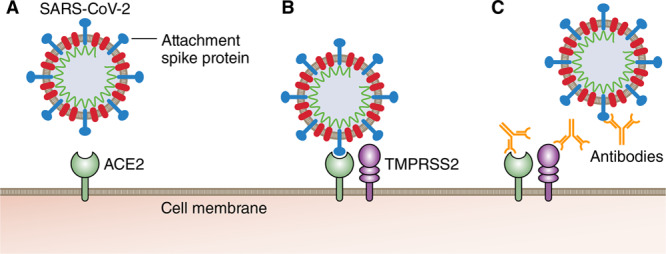
Coronavirus disease 2019 (COVID-19) is a rapidly expanding global pandemic caused by severe acute respiratory syndrome coronavirus 2, resulting in significant morbidity and mortality. A substantial minority of patients hospitalized develop an acute COVID-19 cardiovascular syndrome, which can manifest with a variety of clinical presentations but often presents as an acute cardiac injury with cardiomyopathy, ventricular arrhythmias, and hemodynamic instability in the absence of obstructive coronary artery disease. The cause of this injury is uncertain but is suspected to be related to myocarditis, microvascular injury, systemic cytokine-mediated injury, or stress-related cardiomyopathy. Although histologically unproven, severe acute respiratory syndrome coronavirus 2 has the potential to directly replicate within cardiomyocytes and pericytes, leading to viral myocarditis. Systemically elevated cytokines are also known to be cardiotoxic and have the potential to result in profound myocardial injury. Prior experience with severe acute respiratory syndrome coronavirus 1 has helped expedite the evaluation of several promising therapies, including antiviral agents, interleukin-6 inhibitors, and convalescent serum. Management of acute COVID-19 cardiovascular syndrome should involve a multidisciplinary team including intensive care specialists, infectious disease specialists, and cardiologists. Priorities for managing acute COVID-19 cardiovascular syndrome include balancing the goals of minimizing healthcare staff exposure for testing that will not change clinical management with early recognition of the syndrome at a time point at which intervention may be most effective. This article aims to review the best available data on acute COVID-19 cardiovascular syndrome epidemiology, pathogenesis, diagnosis, and treatment. From these data, we propose a surveillance, diagnostic, and management strategy that balances potential patient risks and healthcare staff exposure with improvement in meaningful clinical outcomes.
2019 年冠状病毒病(COVID-19)是由严重急性呼吸系统综合征冠状病毒 2 引起的迅速蔓延的全球大流行疾病,导致发病率和死亡率显著升高。少数住院患者会出现急性 COVID-19 心血管综合征,其临床表现多样,但通常表现为无阻塞性冠状动脉疾病的急性心脏损伤、心肌病、室性心律失常和血流动力学不稳定。这种损伤的原因尚不确定,但怀疑与心肌炎、微血管损伤、全身细胞因子介导的损伤或应激性心肌病有关。尽管在组织学上尚未得到证实,但严重急性呼吸系统综合征冠状病毒 2 有可能在心肌细胞和周细胞内直接复制,导致病毒性心肌炎。系统中升高的细胞因子也已知具有心脏毒性,并有可能导致严重的心肌损伤。对严重急性呼吸系统综合征冠状病毒 1 的先前经验有助于加速评估几种有前途的治疗方法,包括抗病毒药物、白细胞介素 6 抑制剂和恢复期血清。急性 COVID-19 心血管综合征的管理应包括一个多学科团队,包括重症监护专家、传染病专家和心脏病专家。管理急性 COVID-19 心血管综合征的优先事项包括平衡旨在尽量减少不会改变临床管理的检测所需的医护人员暴露的目标,以及在干预可能最有效的时间点及早识别该综合征。本文旨在回顾急性 COVID-19 心血管综合征的最佳现有流行病学、发病机制、诊断和治疗数据。基于这些数据,我们提出了一种监测、诊断和管理策略,平衡了潜在患者风险和医护人员暴露与改善有意义的临床结局。