Rühle Alexander, Sprave Tanja, Kalckreuth Tobias, Stoian Raluca, Haehl Erik, Zamboglou Constantinos, Laszig Roland, Knopf Andreas, Grosu Anca-Ligia, Nicolay Nils H
Department of Radiation Oncology, University of Freiburg - Medical Center, Faculty of Medicine, Robert-Koch-Str. 3, 79106, Freiburg, Germany.
German Cancer Consortium (DKTK) Partner Site Freiburg, German Cancer Research Centre (DKFZ), Heidelberg, Germany.
Radiat Oncol. 2020 Apr 16;15(1):81. doi: 10.1186/s13014-020-01531-5.
Treatment for local and locoregional recurrence or second head-and-neck (H&N) cancers after previous radiotherapy is challenging, and re-irradiation carries a significantly increased risk for radiotherapy-related normal tissue toxicities and treatment failure due to a radioresistant tumor phenotype. Here, we analyzed re-irradiation management and outcomes in patients with recurrent or second primary H&N carcinoma using state-of-the-art diagnostic procedures and radiotherapy techniques.
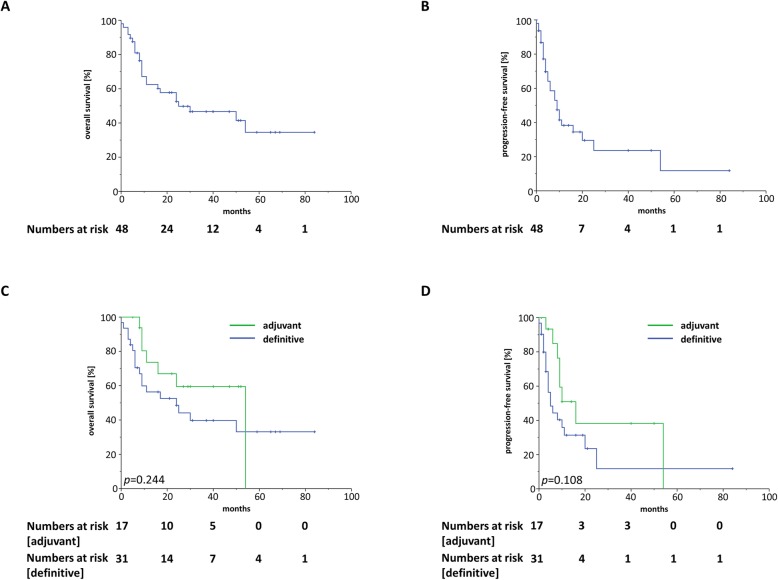
Between 2010 and 2019, 48 patients with recurrent or second primary H&N carcinoma received re-radiotherapy at the University of Freiburg Medical Center and were included in this study. Overall survival (OS) and progression-free survival (PFS) were calculated with the Kaplan-Meier method, and univariate Cox-regression analyses were performed to assess the effects of clinico-pathological factors on treatment outcomes. Acute and chronic treatment-related toxicities were quantified using the Common Terminology Criteria for Adverse Events (CTCAE v4.03).
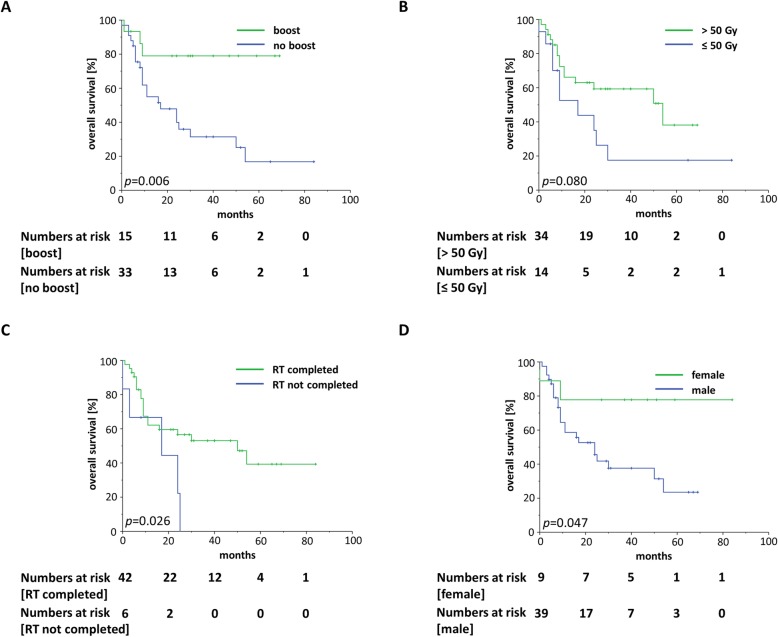
Thirty-one patients (64.6%) received definitive and 17 (35.4%) adjuvant radiotherapy. Simultaneous chemotherapy was administered in 28 patients (58.3%) with cetuximab as the most commonly used systemic agent (n = 17, 60.7%). After a median time of 17 months (range 4 months to 176 months) between first and second radiotherapy, patients were re-irradiated with a median of 58.4 Gy and a treatment completion rate of 87.5% (n = 42). Median OS was 25 months with a 1-year OS amounting to 62.4%, and median PFS was 9 months with a 1-year PFS of 37.6%. Univariate analyses demonstrated that both a lower rT-status and a radiotherapy boost were associated with improved OS (p < 0.05). There was a trend towards superior OS for patients who received > 50 Gy (p = 0.091) and who completed the prescribed radiotherapy (p = 0.055). Five patients (10.4%) suffered from at least one grade 3 toxicities, while 9 patients (27.3%) experienced chronic higher-grade toxicities (≥ grade 3) with one (3.0%) grade 4 carotid blowout and one (3.0%) grade 4 osteoradionecrosis.
Re-irradiation of recurrent or second primary H&N cancer with modern radiation techniques such as intensity-modulated radiotherapy resulted in promising survival rates with acceptable toxicities compared to historical cohorts. Increased re-irradiation doses, utilization of a radiotherapy boost and completion of the re-irradiation treatment were found to result in improved survival.
既往接受过放疗的局部及区域复发或第二原发性头颈部(H&N)癌的治疗具有挑战性,再次放疗会显著增加放疗相关正常组织毒性及因肿瘤放射抗拒表型导致治疗失败的风险。在此,我们使用先进的诊断程序和放疗技术分析了复发性或第二原发性H&N癌患者的再次放疗管理及结果。
2010年至2019年间,48例复发性或第二原发性H&N癌患者在弗莱堡大学医学中心接受了再次放疗,并纳入本研究。采用Kaplan-Meier法计算总生存期(OS)和无进展生存期(PFS),并进行单因素Cox回归分析以评估临床病理因素对治疗结果的影响。使用不良事件通用术语标准(CTCAE v4.03)对急性和慢性治疗相关毒性进行量化。
31例患者(64.6%)接受了根治性放疗,17例(35.4%)接受了辅助放疗。28例患者(58.3%)同时接受了化疗,其中西妥昔单抗是最常用的全身治疗药物(n = 17,60.7%)。首次放疗和第二次放疗的中位间隔时间为17个月(范围4个月至176个月),患者再次放疗的中位剂量为58.4 Gy,治疗完成率为87.5%(n = 42)。中位OS为25个月,1年OS率为62.4%,中位PFS为9个月,1年PFS率为37.6%。单因素分析表明,较低的rT分期和放疗增敏均与OS改善相关(p < 0.05)。接受> 50 Gy放疗的患者(p = 0.091)和完成规定放疗的患者(p = 0.055)的OS有改善趋势。5例患者(10.4%)出现至少1次3级毒性反应,9例患者(27.3%)出现慢性高级别毒性反应(≥ 3级),其中1例(3.0%)发生4级颈动脉破裂,1例(3.0%)发生4级骨放射性坏死。
与历史队列相比,采用强度调制放疗等现代放疗技术对复发性或第二原发性H&N癌进行再次放疗可获得有前景的生存率且毒性可接受。发现增加再次放疗剂量、使用放疗增敏及完成再次放疗治疗可改善生存率。