Fordham Ric, Dhatariya Ketan, Stancliffe Rachel, Lloyd Adam, Chatterjee Mou, Mathew Mevin, Taneja Loveleen, Gains Mike, Haagen Panton Ulrik
The Health Economics Group, University of East Anglia Norwich Medical School, Norwich, UK.
Elsie Bertram Diabetes Centre, Norfolk and Norwich University Hospitals NHS Foundation Trust, Norwich, UK
BMJ Open Diabetes Res Care. 2020 Apr;8(1). doi: 10.1136/bmjdrc-2019-001017.
The management of diabetes-related complications accounts for a large share of total carbon dioxide equivalent (COe) emissions. We assessed whether improving diabetes control in people with type 2 diabetes reduces COe emissions, compared with those with unchanging glycemic control.
Using the IQVIA Core Diabetes Model, we estimated the impact of maintaining glycated hemoglobin (HbA) at 7% (53 mmol/mol) or reducing it by 1% (11 mmol/mol) on total COe/patient and COe/life-year (LY). Two different cohorts were investigated: those on first-line medical therapy (cohort 1) and those on third-line therapy (cohort 2). COe was estimated using cost inputs converted to carbon inputs using the UK National Health Service's carbon intensity factor. The model was run over a 50-year time horizon, discounting total costs and quality adjusted life years (QALYs) up to 5% and COe at 0%.
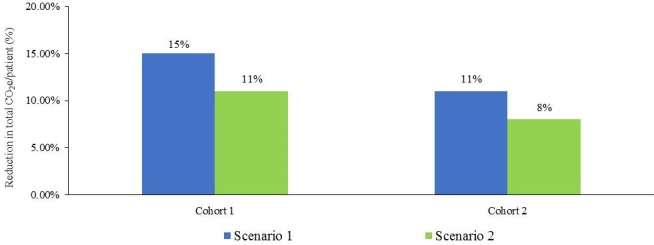
Maintaining HbA at 7% (53 mmol/mol) reduced total COe/patient by 18% (1546 kgCOe/patient) vs 13% (937 kgCOe/patient) in cohorts 1 and 2, respectively, and led to a reduction in COe/LY gain of 15%-20%. Reducing HbA by 1% (11 mmol/mol) caused a 12% (cohort 1) and 9% (cohort 2) reduction in COe/patient with a COe/LY gain reduction of 11%-14%.
When comparing people with untreated diabetes, maintaining glycemic control at 7% (53 mmol/mol) on a single agent or improving HbA by 1% (11 mmol/mol) by the addition of more glucose-lowering treatment was associated with a reduction in carbon emissions.
糖尿病相关并发症的管理在二氧化碳当量(COe)排放总量中占很大比例。我们评估了与血糖控制不变的2型糖尿病患者相比,改善血糖控制是否能减少COe排放。
使用艾昆纬核心糖尿病模型,我们估计了将糖化血红蛋白(HbA)维持在7%(53 mmol/mol)或将其降低1%(11 mmol/mol)对每位患者的总COe以及每生命年(LY)的COe的影响。研究了两个不同的队列:一线药物治疗患者(队列1)和三线治疗患者(队列2)。使用英国国家医疗服务体系的碳强度因子将成本投入转换为碳投入来估算COe。该模型在50年的时间范围内运行,总成本和质量调整生命年(QALY)按最高5%进行贴现,COe按0%进行贴现。
在队列1和队列2中,将HbA维持在7%(53 mmol/mol)分别使每位患者的总COe降低了18%(1546 kgCOe/患者)和13%(937 kgCOe/患者),并使每获得一个LY的COe降低了15% - 20%。将HbA降低1%(11 mmol/mol)使每位患者的COe降低了12%(队列1)和9%(队列2),每获得一个LY的COe降低了11% - 14%。
与未治疗的糖尿病患者相比,使用单一药物将血糖控制维持在7%(53 mmol/mol)或通过增加更多降糖治疗使HbA改善1%(11 mmol/mol)与碳排放减少相关。