Department of Inflammation and Immunity, Cleveland Clinic, Cleveland, OH, USA.
Respiratory Institute, Cleveland Clinic, Cleveland, OH, USA.
Clin Nutr. 2020 Dec;39(12):3711-3720. doi: 10.1016/j.clnu.2020.03.032. Epub 2020 Apr 3.
BACKGROUND & AIMS: There are very limited data on the healthcare burden of muscle loss, the most frequent complication in hospitalized cirrhotics. We determined the healthcare impact of a muscle loss phenotype in hospitalized cirrhotics.
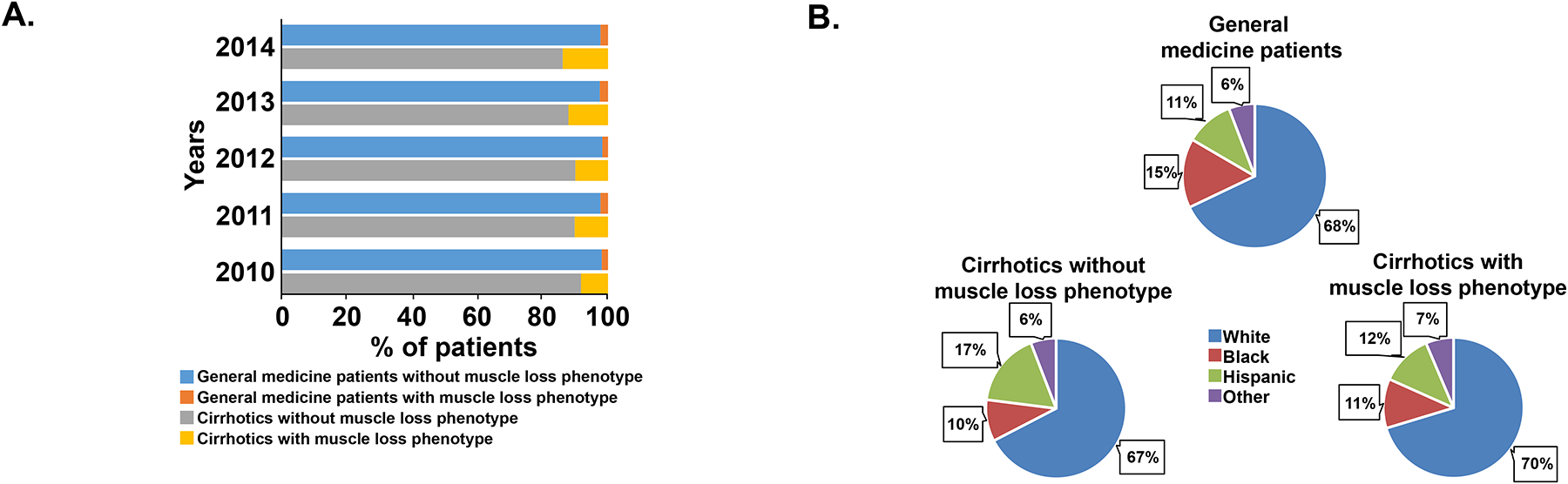
The Nationwide Inpatient Sample (NIS) database (years 2010-2014) was analyzed. Search terms included cirrhosis and its complications, and an expanded definition of a muscle loss phenotype that included all conditions associated with muscle loss. In-hospital mortality, length of stay (LOS), post-discharge disposition, co-morbidities and cost during admission were analyzed. Univariate and multivariate analyses were performed to identify associations between a muscle loss phenotype and outcomes. Impact of muscle loss in cirrhotics was compared to that in a random sample (2%) of general medical inpatients.
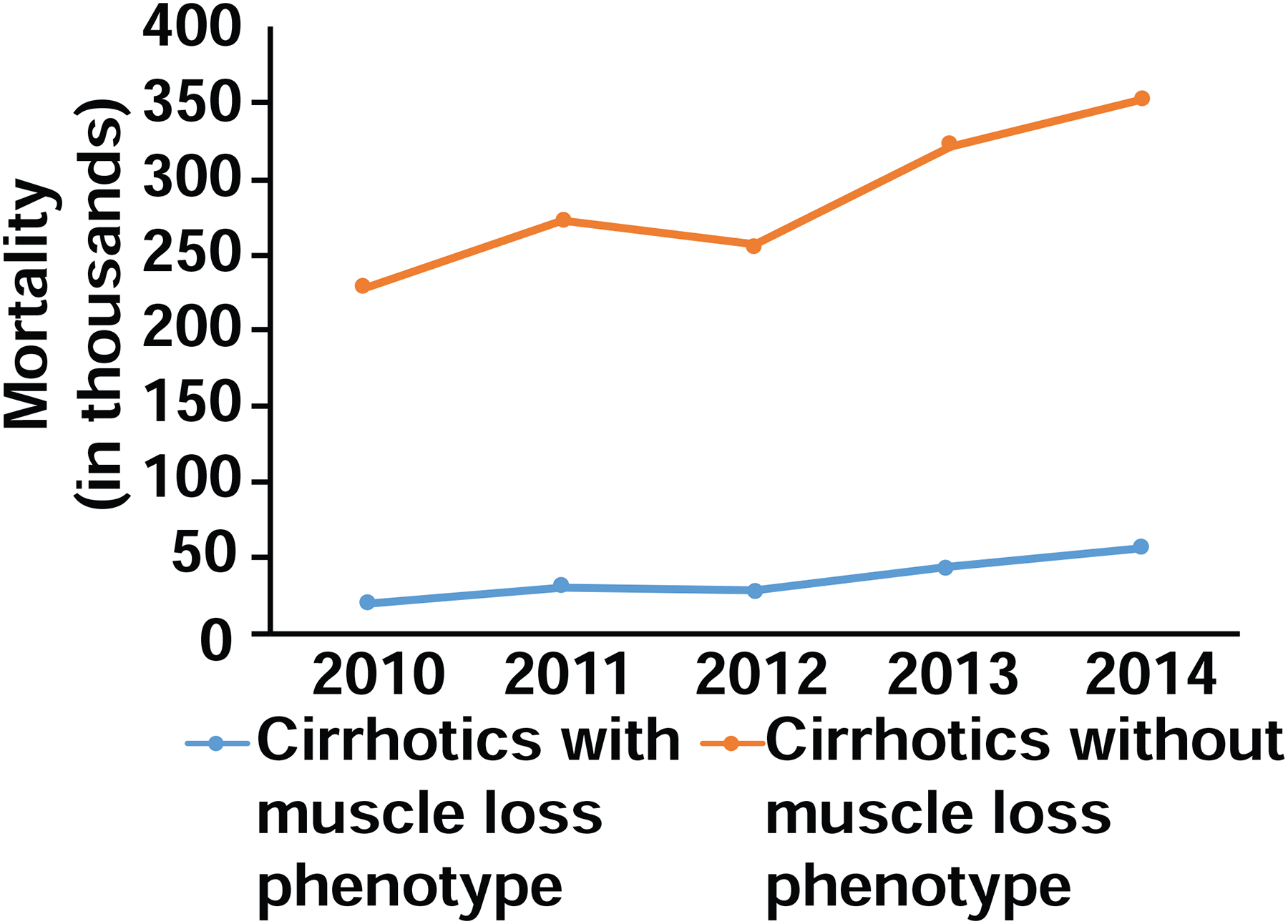
A total of 162,694 hospitalizations for cirrhosis were reported, of which 18,261 (11.2%) included secondary diagnosis codes for a muscle loss phenotype. A diagnosis of muscle loss was associated with a significantly (p < 0.001 for all) higher mortality (19.3% vs 8.2%), LOS (14.2 ± 15.8 vs. 4.6 ± 6.9 days), and median hospital charge per admission ($21,400 vs. $8573) and a lower likelihood of discharge to home (30.1% vs. 60.2%). All evaluated outcomes were more severe in cirrhotics than general medical patients (n = 534,687). Multivariate regression analysis showed that a diagnosis of muscle loss independently increased mortality by 130%, LOS by 80% and direct cost of care by 119% (p < 0.001 for all). Alcohol use, female gender, malignancies and other organ dysfunction were independently associated with muscle loss.
Muscle loss contributed to higher mortality, LOS, and direct healthcare costs in hospitalized cirrhotics.
肌肉减少症是住院肝硬化患者最常见的并发症,但目前关于其对医疗保健的影响的数据非常有限。本研究旨在确定住院肝硬化患者中肌肉减少表型的医疗保健影响。
分析了全国住院患者样本(NIS)数据库(2010-2014 年)。检索词包括肝硬化及其并发症,以及肌肉减少表型的扩展定义,其中包括所有与肌肉减少相关的疾病。分析了住院期间的院内死亡率、住院时间(LOS)、出院后去向、合并症和入院费用。采用单变量和多变量分析来确定肌肉减少表型与结局之间的关系。将肝硬化患者的肌肉减少症的影响与一般内科住院患者的随机样本(2%)进行比较。
报告了 162694 例肝硬化住院患者,其中 18261 例(11.2%)包括肌肉减少表型的次要诊断代码。诊断为肌肉减少与死亡率显著升高(19.3% vs. 8.2%,p < 0.001)、住院时间(14.2 ± 15.8 天 vs. 4.6 ± 6.9 天)、住院费用中位数(21400 美元 vs. 8573 美元)以及出院回家的可能性降低(30.1% vs. 60.2%)显著相关(p < 0.001)。与一般内科患者相比,肝硬化患者的所有评估结果均更为严重(n = 534687)。多变量回归分析显示,肌肉减少症的诊断使死亡率独立增加了 130%,住院时间延长了 80%,直接医疗费用增加了 119%(p < 0.001)。饮酒、女性、恶性肿瘤和其他器官功能障碍与肌肉减少症独立相关。
肌肉减少症导致住院肝硬化患者的死亡率、住院时间和直接医疗保健费用增加。