Department of Translational Molecular Pathology, University of Texas MD Anderson Cancer Center, Houston, TX, USA
Department of Investigational Cancer Therapeutics, University of Texas MD Anderson Cancer Center, Houston, TX, USA.
J Immunother Cancer. 2020 Apr;8(1). doi: 10.1136/jitc-2020-000665.
Decreased tumor content (TC) in resection specimens after neoadjuvant therapy is used to predict prognosis. We investigated whether TC assessed in biopsy specimens or the shift in TC from baseline to on-treatment can be used accordingly to predict response in patients with rare tumors who were treated with pembrolizumab.
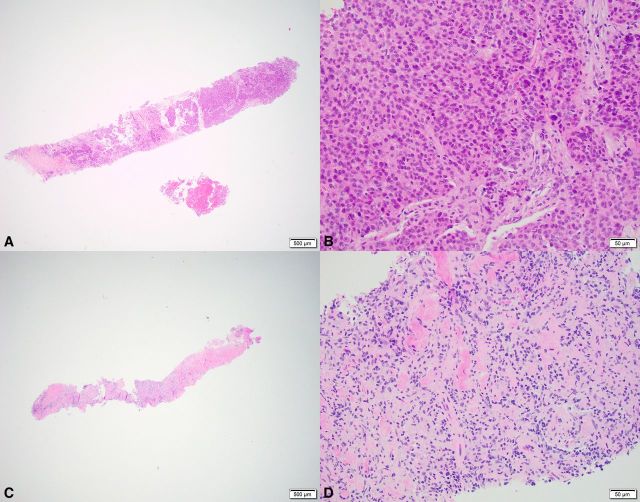
A total of 57 tumors (represented by 173 baseline and 179 on-treatment biopsies) from 57 patients with rare tumors participating in an ongoing phase II clinical trial of pembrolizumab were evaluated. TC was estimated on H&E-stained slides and tumors were dichotomized into low and high TC according to a cut-off of 10%. Necrosis, proliferative fibrosis (PF) and normal tissue were assessed in on-treatment biopsies. TC at baseline and on-treatment, as well as the shift in TC from baseline to on-treatment, was correlated with clinical response defined according to Response Evaluation Criteria in Solid Tumors.
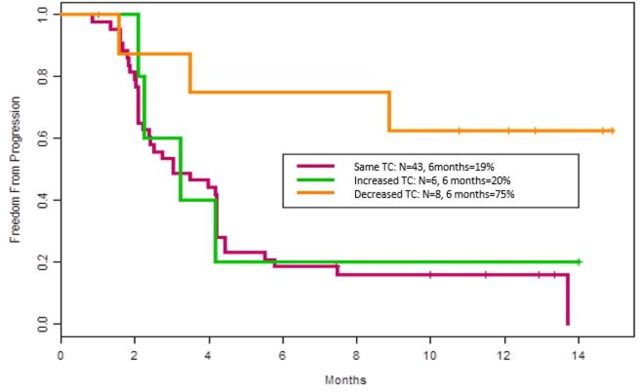
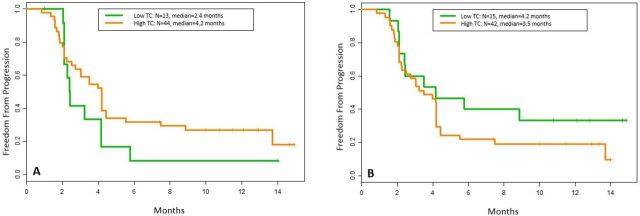
A decrease in TC was seen in 14% (n=8); no change in TC was seen in 75% (n=43); and an increase in TC from baseline to on-treatment was seen in 11% (n=6). Objective response was significantly associated with decrease in TC from baseline to on-treatment (38%, 3/8) compared with no change/increase in TC (6%, 3/49) (p=0.031). Patients with a decrease in TC had a significantly increased time to progression (TTP) (75% probability) compared with patients with an increase (20% probability) or no change in TC (19% probability) (p=0.0042). Low TC was seen in 23% (13/57) of the tumors at baseline and in 26% (15/57) on-treatment. High TC was seen in 77% (44/57) of tumors at baseline and in 74% (42/57) on-treatment. No significant associations with response were seen for necrosis, PF or normal tissue in on-treatment biopsies.
Patients with a decrease in TC from baseline to on-treatment had a significant improvement in objective response and a longer TTP. Our data suggest that the shift in TC might be used to predict response to pembrolizumab in rare tumors. However, further investigations in larger cohorts are needed to determine the clinical value of TC, the shift in TC and the cut-off of 10% assessed in biopsies.
NCT02721732.
新辅助治疗后切除标本中的肿瘤含量(TC)降低可用于预测预后。我们研究了在接受 pembrolizumab 治疗的罕见肿瘤患者中,评估活检标本中的 TC 或 TC 从基线到治疗期间的变化是否可以相应地预测反应。
共评估了 57 名罕见肿瘤患者的 57 个肿瘤(代表 173 个基线和 179 个治疗期间活检),这些患者参加了 pembrolizumab 的一项正在进行的 II 期临床试验。在 H&E 染色切片上估计 TC,并根据 10%的截止值将肿瘤分为低 TC 和高 TC。评估治疗期间活检中的坏死、增殖性纤维化(PF)和正常组织。TC 基线和治疗期间,以及 TC 从基线到治疗期间的变化与根据实体瘤反应评价标准定义的临床反应相关。
TC 降低见于 14%(n=8);TC 无变化见于 75%(n=43);基线至治疗期间 TC 增加见于 11%(n=6)。与 TC 无变化/增加(6%,3/49)相比,TC 从基线到治疗期间的降低与客观缓解显著相关(38%,3/8)(p=0.031)。与 TC 增加(20%,概率)或 TC 无变化(19%,概率)的患者相比,TC 降低的患者进展时间(TTP)显著增加(75%的概率)(p=0.0042)。基线时,13%(57 例中的 13 例)肿瘤中 TC 较低,治疗时为 26%(57 例中的 15 例)。基线时,77%(57 例中的 44 例)肿瘤中 TC 较高,治疗时为 74%(57 例中的 42 例)。治疗期间活检中未见坏死、PF 或正常组织与反应显著相关。
TC 从基线到治疗期间降低的患者客观缓解和 TTP 显著改善。我们的数据表明,TC 的变化可能用于预测罕见肿瘤对 pembrolizumab 的反应。然而,需要在更大的队列中进行进一步研究,以确定活检中 TC、TC 变化和 10%的截止值的临床价值。
NCT02721732。