Division of Cardiology Dartmouth-Hitchcock Medical Center Geisel School of Medicine at Dartmouth Lebanon NH.
Division of Cardiology Massachusetts General Hospital Boston MA.
J Am Heart Assoc. 2020 Apr 21;9(8):e014738. doi: 10.1161/JAHA.119.014738. Epub 2020 Apr 20.
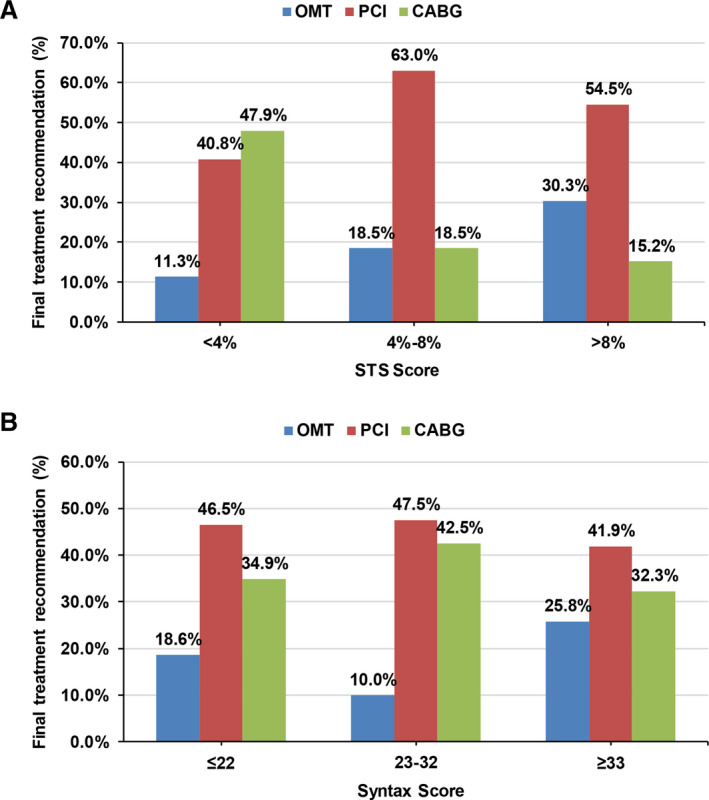
Background The Heart Team approach is ascribed a Class I recommendation in contemporary guidelines for revascularization of complex coronary artery disease. However, limited data are available regarding the decision-making and outcomes of patients based on this strategy. Methods and Results One hundred sixty-six high-risk coronary artery disease patients underwent Heart Team evaluation at a single institution between January 2015 and November 2018. We prospectively collected data on demographics, symptoms, Society of Thoracic Surgeons Predicted Risk of Mortality/Synergy Between PCI with Taxus and Cardiac Surgery (STS-PROM/SYNTAX) scores, mode of revascularization, and outcomes. Mean age was 70.0 years; 122 (73.5%) patients were male. Prevalent comorbidities included diabetes mellitus (51.8%), peripheral artery disease (38.6%), atrial fibrillation (27.1%), end-stage renal disease on dialysis (13.3%), and chronic obstructive pulmonary disease (21.7%). Eighty-seven (52.4%) patients had New York Heart Association III-IV and 112 (67.5%) had Canadian Cardiovascular Society III-IV symptomatology. Sixty-seven (40.4%) patients had left main and 118 (71.1%) had 3-vessel coronary artery disease. The median STS-PROM was 3.6% (interquartile range 1.9, 8.0) and SYNTAX score was 26 (interquartile range 20, 34). The median number of physicians per Heart Team meeting was 6 (interquartile range 5, 8). Seventy-nine (47.6%) and 49 (29.5%) patients underwent percutaneous coronary intervention and coronary artery bypass grafting, respectively. With increasing STS-PROM (low, intermediate, high operative risk), coronary artery bypass graft was performed less often (47.9%, 18.5%, 15.2%) and optimal medical therapy was recommended more often (11.3%, 18.5%, 30.3%). There were no trends in recommendation for coronary artery bypass graft, percutaneous coronary intervention, or optimal medical therapy by SYNTAX score tertiles. In-hospital and 30-day mortality was 3.9% and 4.8%, respectively. Conclusions Integrating a multidisciplinary Heart Team into institutional practice is feasible and provides a formalized approach to evaluating complex coronary artery disease patients. The comprehensive assessment of surgical, anatomical, and other risk scores using a decision aid may guide appropriate, evidence-based management within this team-based construct.
心脏团队方法在当代复杂冠状动脉疾病血运重建的指南中被归为 I 类推荐。然而,关于基于这种策略的患者决策和结果的数据有限。
在一家单中心医院,166 名高危冠状动脉疾病患者在 2015 年 1 月至 2018 年 11 月期间接受了心脏团队评估。我们前瞻性地收集了人口统计学、症状、胸外科医师协会预测死亡率/紫杉醇与心脏手术的协同作用评分(STS-PROM/SYNTAX)、血运重建方式和结果的数据。平均年龄为 70.0 岁;122 名(73.5%)患者为男性。常见合并症包括糖尿病(51.8%)、外周动脉疾病(38.6%)、心房颤动(27.1%)、终末期肾脏病透析(13.3%)和慢性阻塞性肺疾病(21.7%)。87 名(52.4%)患者为纽约心脏协会 III-IV 级,112 名(67.5%)患者为加拿大心血管学会 III-IV 级症状。67 名(40.4%)患者有左主干病变,118 名(71.1%)患者有 3 支血管病变。STS-PROM 的中位数为 3.6%(四分位距 1.9,8.0),SYNTAX 评分为 26(四分位距 20,34)。每次心脏团队会议的平均医生人数为 6 人(四分位距 5,8)。79 名(47.6%)和 49 名(29.5%)患者分别接受了经皮冠状动脉介入治疗和冠状动脉旁路移植术。随着 STS-PROM(低、中、高手术风险)的增加,冠状动脉旁路移植术的应用越来越少(47.9%、18.5%、15.2%),而最佳药物治疗的推荐越来越多(11.3%、18.5%、30.3%)。根据 SYNTAX 评分三分位数,冠状动脉旁路移植术、经皮冠状动脉介入治疗或最佳药物治疗的推荐没有趋势。住院期间和 30 天死亡率分别为 3.9%和 4.8%。
将多学科心脏团队纳入机构实践是可行的,并为评估复杂冠状动脉疾病患者提供了一种规范化的方法。使用决策辅助工具综合评估手术、解剖和其他风险评分,可能有助于在这种基于团队的结构中进行适当的、基于证据的管理。