National Heart Lung Institute, Imperial College London, London SW3 6LR, UK.
London School of Hygiene and Tropical Medicine, London, UK.
Int J Chron Obstruct Pulmon Dis. 2020 Apr 2;15:701-710. doi: 10.2147/COPD.S241568. eCollection 2020.
Inhaled corticosteroids (ICS) are a prevailing treatment option for COPD patients but recent guidelines have relegated their use predominantly to patients with frequent exacerbations. Yet large numbers of patients worldwide are currently treated with ICS-containing regimens. We wished to determine in routine clinical practice how common ICS withdrawal is and the differences in health outcomes between patients managed on ICS-containing and non-ICS containing regimens.
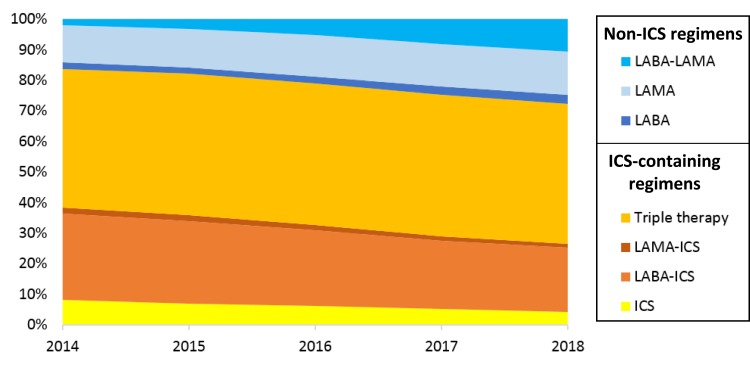
COPD patients were identified from the UK primary care electronic healthcare records, between 2014 and 2018. Patients were grouped into three treatment regimens: long-acting beta-agonist (LABA) and inhaled corticosteroids (ICS), LABA and long-acting muscarinic antagonist (LAMA), and triple therapy (LABA, LAMA and ICS). Annual incidence of ICS withdrawal was measured. Multivariable logistic regression was used to identify patient factors associated with withdrawal. Multivariable Poisson regression was used to assess the association of exacerbations and hospitalised pneumonia between the ICS-containing regimens (LABA-ICS and triple therapy) and patients prescribed LABA-LAMA.
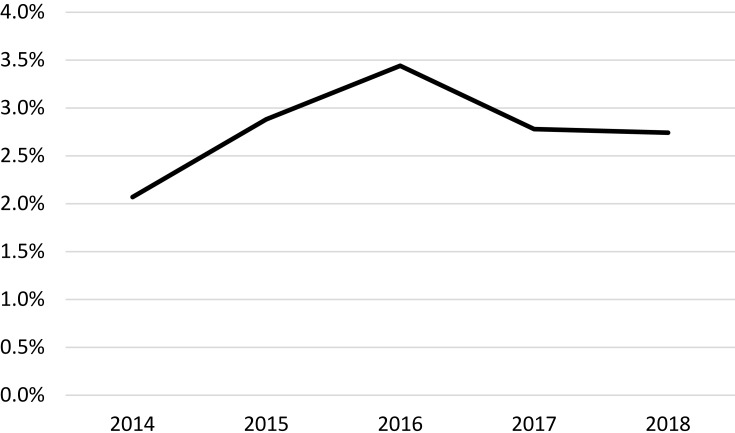
Of 117,046 patients, around three-quarters were prescribed ICS-containing inhalers but ICS withdrawal occurred annually in only approximately 2-3% of patients. Exacerbations in the past year, but not a past history of pneumonia, were associated with ICS withdrawal. A total of 31,034 patients using three treatment regimens (LABA-ICS, LABA-LAMA or triple therapy) were assessed for their relative risk of exacerbations and pneumonia; the exacerbation risk was slightly lower in LABA-ICS users but the same in triple therapy users, as compared to LABA-LAMA users (LABA-ICS adjusted IRR=0.82 (95% CI 0.73-0.93), triple adjusted IRR=0.99 (95% CI 0.88-1.11)). There was no difference in the pneumonia risk (LABA-ICS adjusted IRR=0.96 (95% CI 0.71-1.31), triple adjusted IRR=1.16 (95% CI 0.87-1.57)).
Use of ICS-containing inhaled medication is prevalent across the UK while ICS withdrawal from established treatment was relatively uncommon. Exacerbations and pneumonia risk was similar between the ICS-containing and non-ICS containing treatment regimens.
吸入性皮质类固醇(ICS)是 COPD 患者的主要治疗选择,但最近的指南主要将其用途限于频繁发作的患者。然而,全球仍有大量患者接受含有 ICS 的治疗方案。我们希望在常规临床实践中确定 ICS 停药的常见程度,以及使用含有 ICS 和不含 ICS 的治疗方案的患者在健康结果方面的差异。
在 2014 年至 2018 年间,我们从英国初级保健电子医疗记录中确定了 COPD 患者。患者被分为三种治疗方案:长效β-激动剂(LABA)和吸入性皮质类固醇(ICS)、LABA 和长效毒蕈碱拮抗剂(LAMA)和三联疗法(LABA、LAMA 和 ICS)。测量了 ICS 停药的年发生率。多变量逻辑回归用于确定与停药相关的患者因素。多变量泊松回归用于评估含有 ICS 的方案(LABA-ICS 和三联疗法)和 LABA-LAMA 处方患者之间的发作和住院性肺炎之间的关联。
在 117046 名患者中,约四分之三的患者接受了含有 ICS 的吸入器治疗,但每年只有约 2-3%的患者停用 ICS。过去一年的发作,但没有肺炎病史,与 ICS 停药有关。共评估了 31034 名使用三种治疗方案(LABA-ICS、LABA-LAMA 或三联疗法)的患者的发作和肺炎相对风险;与 LABA-LAMA 患者相比,LABA-ICS 使用者的发作风险略低,而三联疗法使用者的发作风险相同(LABA-ICS 调整后的 IRR=0.82(95%CI 0.73-0.93),三重调整后的 IRR=0.99(95%CI 0.88-1.11))。肺炎风险无差异(LABA-ICS 调整后的 IRR=0.96(95%CI 0.71-1.31),三重调整后的 IRR=1.16(95%CI 0.87-1.57))。
在英国,使用含有 ICS 的吸入药物很普遍,而从既定治疗中停用 ICS 相对较少见。ICS 组和非 ICS 组的发作和肺炎风险相似。