Ding Guang-Yu, Zhu Xiao-Dong, Ji Yuan, Shi Guo-Ming, Shen Ying-Hao, Zhou Jian, Fan Jia, Sun Hui-Chuan, Huang Cheng
Department of Liver Surgery and Transplantation, Liver Cancer Institute, Zhongshan Hospital, Fudan University, Shanghai 200032, China.
Key Laboratory for Carcinogenesis and Cancer Invasion, the Chinese Ministry of Education, Shanghai 200032, China.
Ann Transl Med. 2020 Mar;8(5):204. doi: 10.21037/atm.2020.01.44.
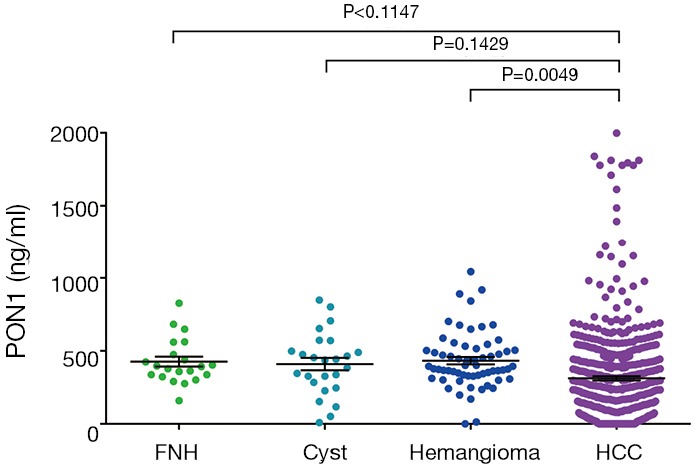
Microvascular invasion (MVI) is considered as one of the most powerful prognostic factors in hepatocellular carcinoma (HCC). Currently, it could only be diagnosed by post-operative histological examination. This study aimed to assess the diagnostic value of serum paraoxonase 1 (PON1) for MVI.
In this study, we analyzed data from 754 HCC patients who underwent surgical treatment between December 2010 and November 2011. Serum PON1 was measured by ELISA and receiver operating characteristic (ROC) curve was applied to calculate diagnostic accuracy.
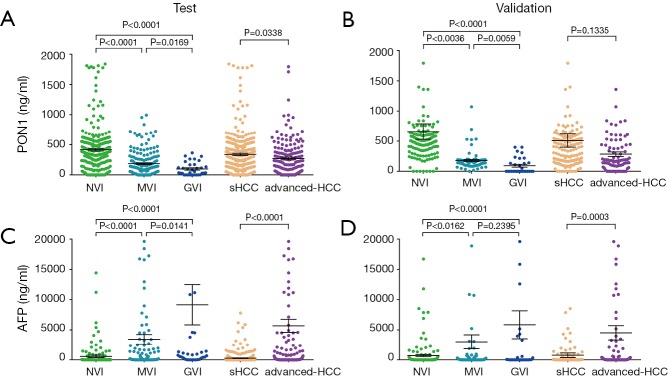
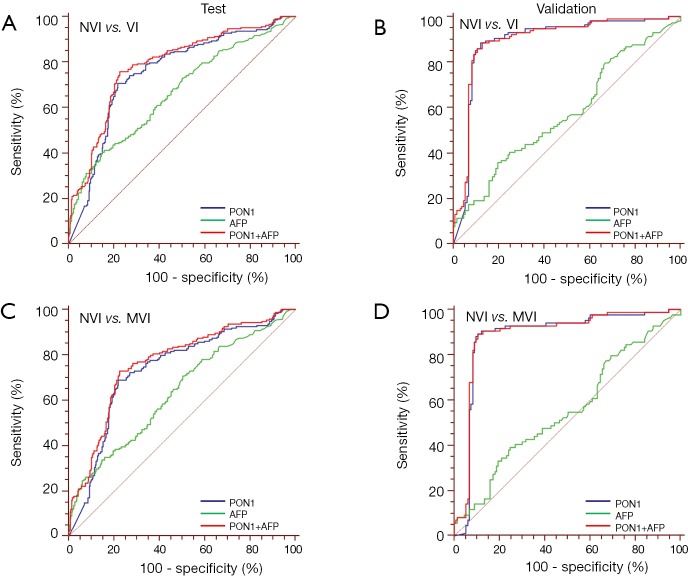
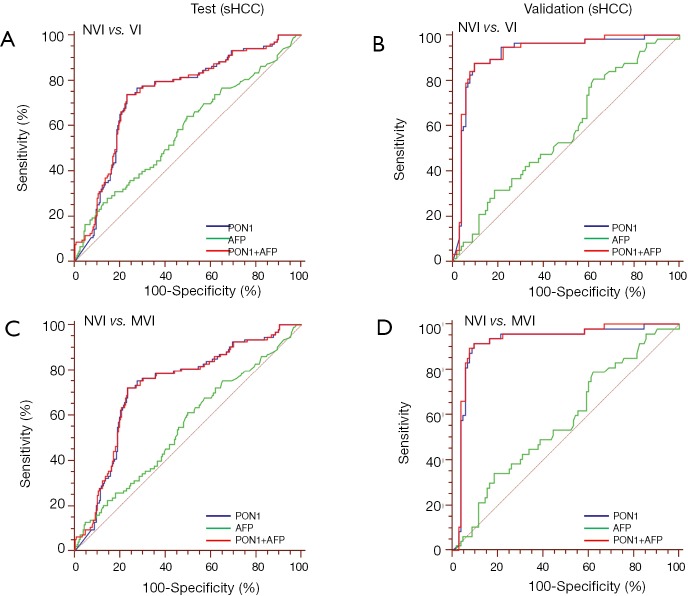
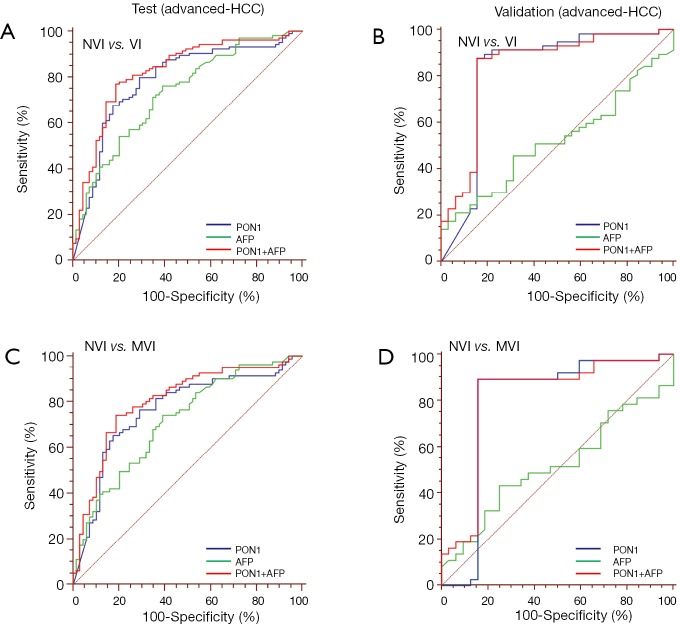
MVI was detected in 174 of 505 patients (34.5%) in the test cohort and 84 of 249 patients (33.7%) in the validation cohort. Univariate analyses indicated tumor size, AFP, and PON1 were significantly related with vascular invasion status. ROC curves determined the optimum diagnostic cutoff value for PON1 was 191.12 ng/mL (AUC 0.754, 95% CI: 0.710-0.798, sensitivity 70.67%, specificity 78.11% in the test cohort), which was significantly better than AFP (cutoff value 279.8 ng/mL, AUC 0.666, 95% CI: 0.618-0.714, sensitivity 40.38%, specificity 85.19%, P=0.0063). In the sHCC sub-group, PON1 retained diagnostic value (AUC 0.738, 95% CI: 0.680-0.796, sensitivity 72.82%, specificity 76.57% in the test cohort), while AFP failed to do so (AUC 0.579, 95% CI: 0.511-0.647, sensitivity 26.21%, specificity 86.84%, P=0.0003). These results were further confirmed by the validation cohort. The combination of PON1 and AFP increased the diagnostic accuracy for vascular invasion compared with either test alone (AUC 0.785, 95% CI: 0.744-0.826, sensitivity 75.96%, specificity 77.44%; PON1 plus AFP . PON1 alone, P=0.0004; PON1 plus AFP AFP alone, P<0.0001).
Serum PON1 could potentially be used to diagnose MVI and could be used to guide more personalized treatment strategy.
微血管侵犯(MVI)被认为是肝细胞癌(HCC)最有力的预后因素之一。目前,它只能通过术后组织学检查来诊断。本研究旨在评估血清对氧磷酶1(PON1)对MVI的诊断价值。
在本研究中,我们分析了2010年12月至2011年11月期间接受手术治疗的754例HCC患者的数据。通过酶联免疫吸附测定(ELISA)法检测血清PON1,并应用受试者工作特征(ROC)曲线计算诊断准确性。
在测试队列的505例患者中有174例(34.5%)检测到MVI,在验证队列的249例患者中有84例(33.7%)检测到MVI。单因素分析表明肿瘤大小、甲胎蛋白(AFP)和PON1与血管侵犯状态显著相关。ROC曲线确定PON1的最佳诊断临界值为191.12 ng/mL(测试队列中曲线下面积[AUC]为0.754,95%置信区间[CI]:0.710 - 0.798,灵敏度70.67%,特异性78.11%),这显著优于AFP(临界值279.8 ng/mL,AUC 0.666,95% CI:0.618 - 0.714,灵敏度40.38%,特异性85.19%,P = 0.0063)。在小肝癌(sHCC)亚组中,PON1保留了诊断价值(测试队列中AUC 0.738,95% CI:0.680 - 0.796,灵敏度72.82%,特异性76.57%),而AFP则未能如此(AUC 0.579,95% CI:0.511 - 0.647,灵敏度26.21%,特异性86.84%,P = 0.0003)。这些结果在验证队列中得到进一步证实。与单独检测相比,PON1和AFP联合检测提高了血管侵犯的诊断准确性(AUC 0.785,95% CI:0.744 - 0.826,灵敏度75.96%,特异性77.44%;PON1加AFP PON1单独检测,P = 0.0004;PON1加AFP AFP单独检测,P < 0.0001)。
血清PON1可能可用于诊断MVI,并可用于指导更个性化的治疗策略。