Department of Medicine, University of Virginia School of Medicine, Charlottesville; Department of Microbiology, University of Virginia School of Medicine, Charlottesville.
Department of Pediatrics, University of Virginia School of Medicine, Charlottesville.
J Allergy Clin Immunol. 2020 Sep;146(3):555-570. doi: 10.1016/j.jaci.2020.03.037. Epub 2020 Apr 19.
Allergic asthmatic subjects are uniquely susceptible to acute wheezing episodes provoked by rhinovirus. However, the underlying immune mechanisms and interaction between rhinovirus and allergy remain enigmatic, and current paradigms are controversial.
We sought to perform a comprehensive analysis of type 1 and type 2 innate and adaptive responses in allergic asthmatic subjects infected with rhinovirus.
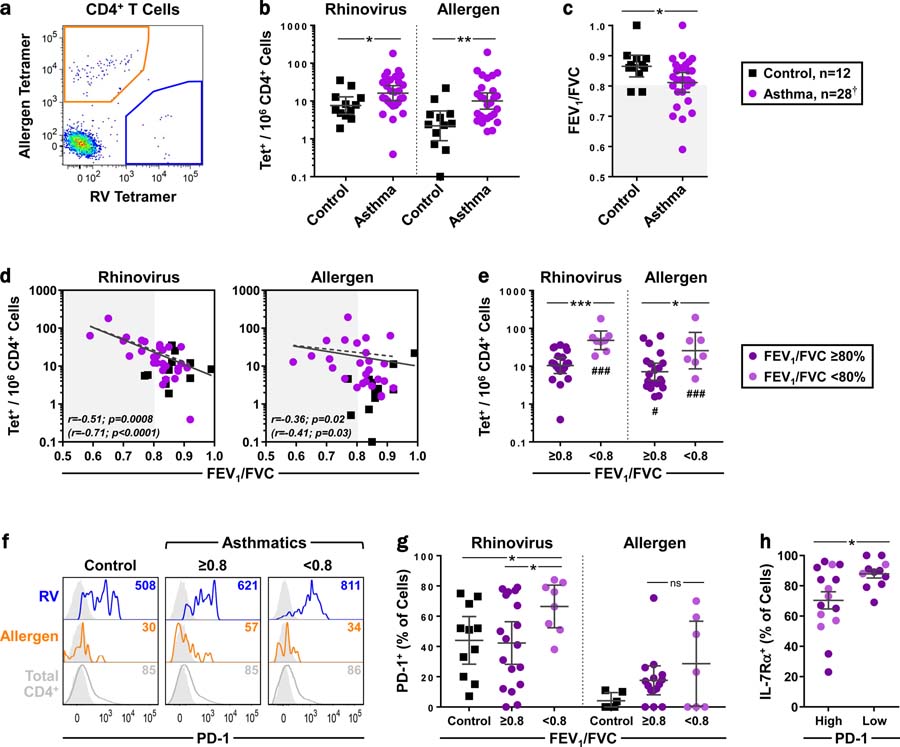
Circulating virus-specific T1 cells and allergen-specific T2 cells were precisely monitored before and after rhinovirus challenge in allergic asthmatic subjects (total IgE, 133-4692 IU/mL; n = 28) and healthy nonallergic controls (n = 12) using peptide/MHCII tetramers. T cells were sampled for up to 11 weeks to capture steady-state and postinfection phases. T-cell responses were analyzed in parallel with 18 cytokines in the nose, upper and lower airway symptoms, and lung function. The influence of in vivo IgE blockade was also examined.
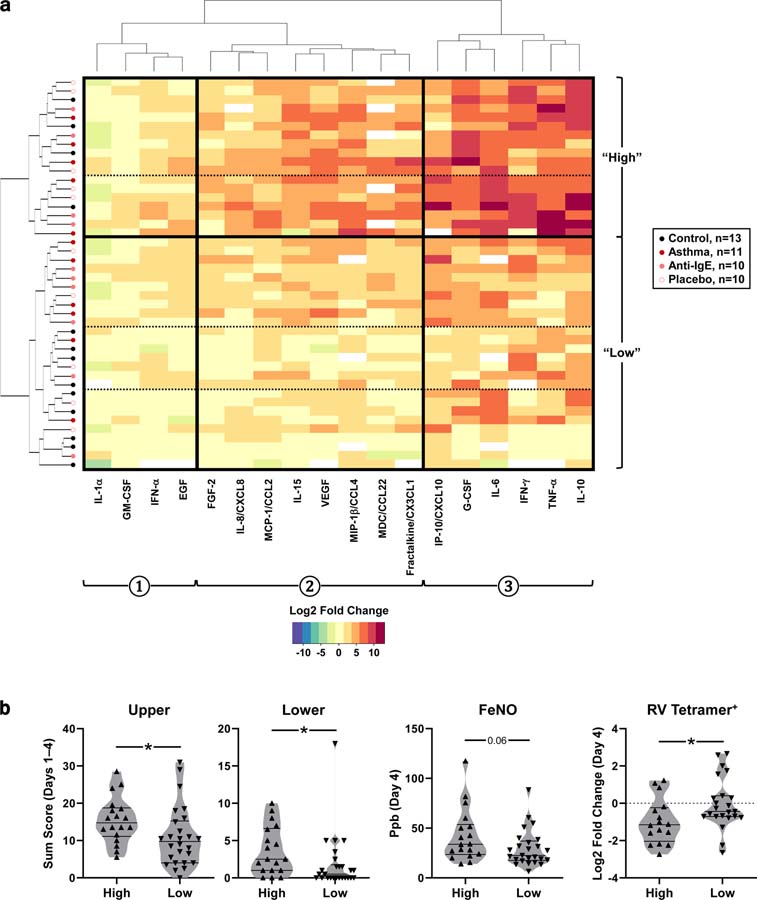
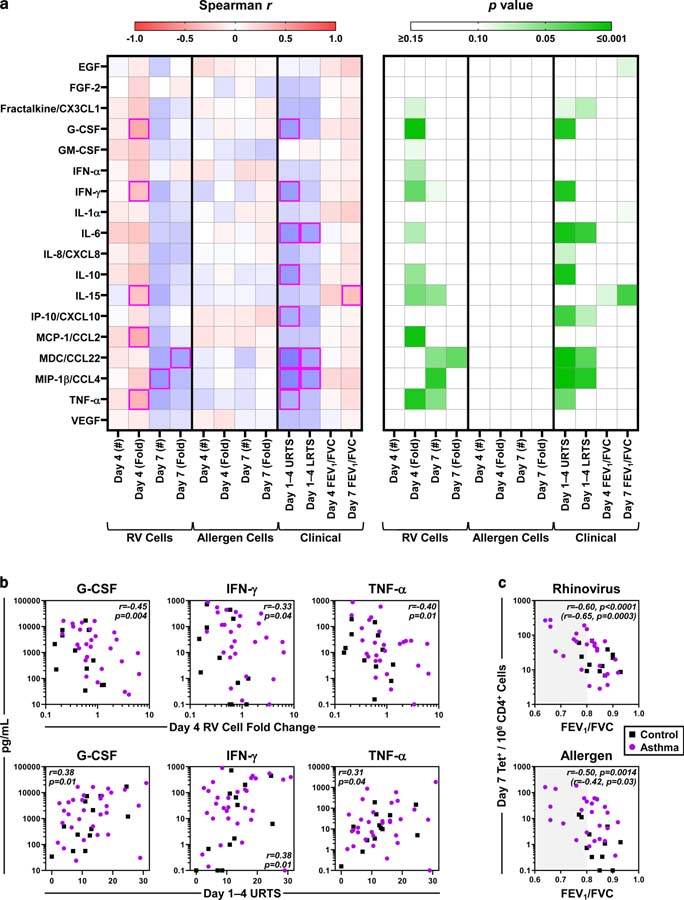
In uninfected asthmatic subjects, higher numbers of circulating virus-specific PD-1 T1 cells, but not allergen-specific T2 cells, were linked to worse lung function. Rhinovirus infection induced an amplified antiviral T1 response in asthmatic subjects versus controls, with synchronized allergen-specific T2 expansion, and production of type 1 and 2 cytokines in the nose. In contrast, T2 responses were absent in infected asthmatic subjects who had normal lung function, and in those receiving anti-IgE. Across all subjects, early induction of a minimal set of nasal cytokines that discriminated high responders (G-CSF, IFN-γ, TNF-α) correlated with both egress of circulating virus-specific T1 cells and worse symptoms.
Rhinovirus induces robust T1 responses in allergic asthmatic subjects that may promote disease, even after the infection resolves.
过敏哮喘患者特别容易受到鼻病毒引发的急性喘息发作的影响。然而,鼻病毒和过敏之间的潜在免疫机制和相互作用仍然是个谜,目前的范式也存在争议。
我们试图对感染鼻病毒的过敏哮喘患者的 1 型和 2 型先天和适应性反应进行全面分析。
使用肽/MHCII 四聚体,在过敏哮喘患者(总 IgE,133-4692IU/mL;n=28)和健康非过敏对照者(n=12)感染鼻病毒前和感染后精确监测循环病毒特异性 T1 细胞和过敏原特异性 T2 细胞。采集 T 细胞样本长达 11 周,以捕获稳态和感染后阶段。同时分析 T 细胞反应与鼻腔、上呼吸道和下呼吸道症状以及肺功能中的 18 种细胞因子。还研究了体内 IgE 阻断的影响。
在未感染的哮喘患者中,循环病毒特异性 PD-1 T1 细胞数量较高,但过敏原特异性 T2 细胞数量较低,与肺功能更差相关。与对照组相比,鼻病毒感染在哮喘患者中诱导了扩增的抗病毒 T1 反应,伴有同步的过敏原特异性 T2 扩增,以及在鼻腔中产生 1 型和 2 型细胞因子。相比之下,在肺功能正常的感染哮喘患者和接受抗 IgE 治疗的患者中,T2 反应缺失。在所有受试者中,早期诱导一组可区分高反应者的最小鼻腔细胞因子(G-CSF、IFN-γ、TNF-α)与循环病毒特异性 T1 细胞的流出和症状恶化相关。
鼻病毒在过敏哮喘患者中诱导强烈的 T1 反应,即使感染消退后,也可能促进疾病。