Defauw Rufin J, Tomšič Anton, van Brakel Thomas J, Marsan Nina Ajmone, Klautz Robert J M, Palmen Meindert
Department of Cardio-Thoracic Surgery, Leiden University Medical Center, Leiden, Netherlands.
Department of Cardiology, Leiden University Medical Center, Leiden, Netherlands.
Eur J Cardiothorac Surg. 2020 Sep 1;58(3):544-550. doi: 10.1093/ejcts/ezaa079.
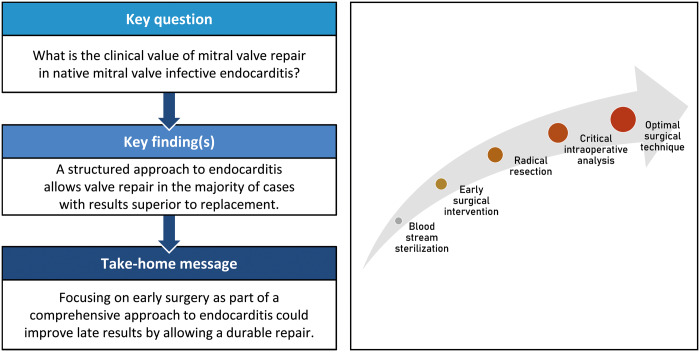
Mitral valve repair in native active infective endocarditis is technically challenging. The survival benefit over valve replacement is poorly established and possibly absent because of the high risk of repair failure and reoperation. In this study, we explore the results of our structured approach in these patients.
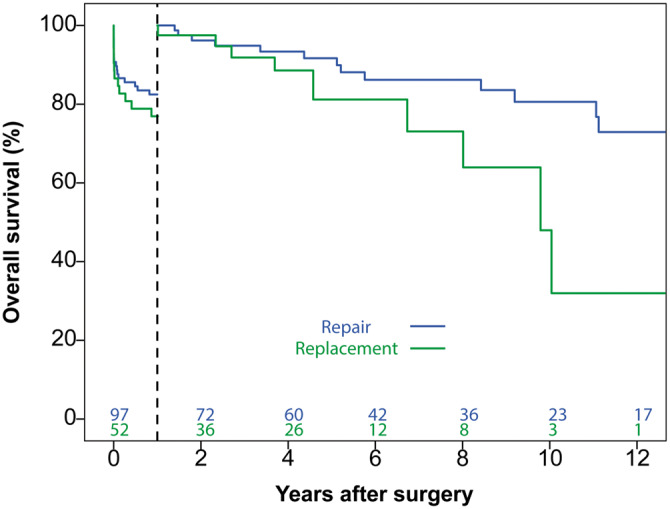
Between January 2000 and January 2017, 149 patients underwent surgery for native mitral infective endocarditis. Among them, 97 (66%) patients underwent valve repair and 52 (34%) underwent valve replacement. Our structured approach consisted of early surgery, radical resection of infected tissue, liberal use of prosthetic materials and 'patch' repair techniques. A critical assessment of expected repair durability was made intraoperatively and repair was not performed if concerns of long-term durability existed. To study the effects of valve repair on overall survival, landmark analysis was performed.
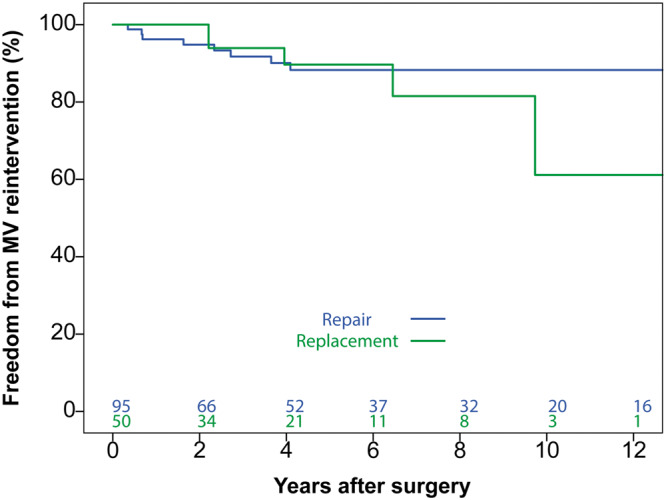
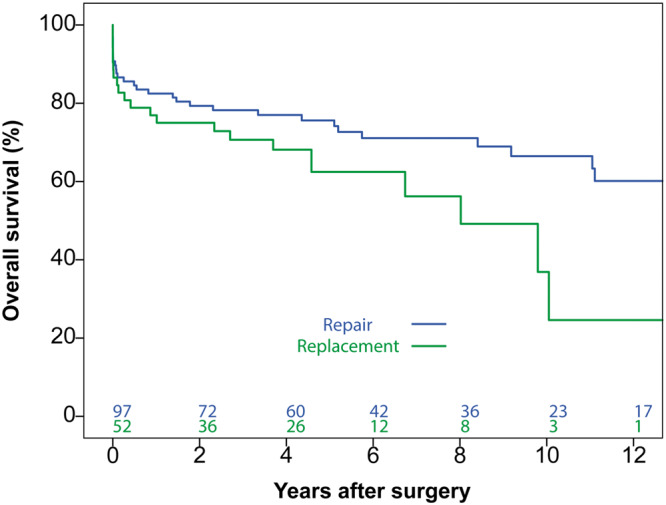
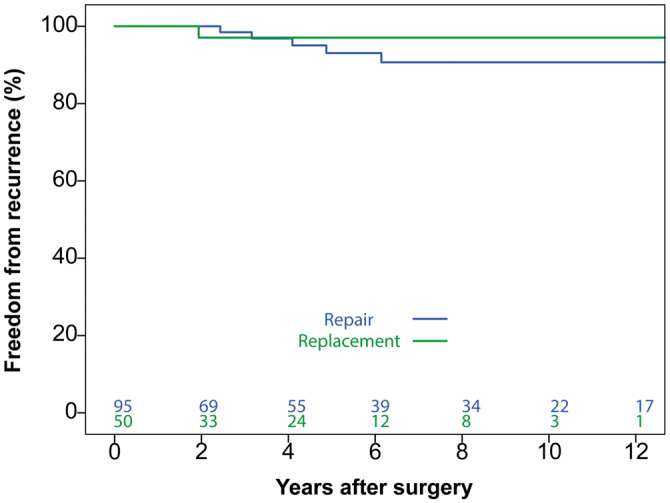
In-hospital mortality was 15.4% (14 repair vs 9 replacement patients; P = 0.642). There were no residual infective endocarditis cases or early reoperations. On Cox proportional hazards analysis, valve replacement was not inferior to repair within 1-year post-surgery [hazard ratio (HR) 1.134, 95% confidence interval (CI) 0.504-2.540; P = 0.76]. Beyond 1 year post-surgery, replacement was associated with decreased survival (HR 2.534, 95% CI 1.002-6.406; P = 0.049). There were no differences in freedom from recurrent infective endocarditis (P = 0.47) and mitral valve reintervention (P = 0.52).
Active mitral valve endocarditis remains a complex disease with significant early and late morbidity and mortality. A structured approach allows valve repair in two-thirds of patients. Clinical results could be improved by focussing on early surgery, prior to extensive valve destruction, to enable durable repairs and improve late outcomes.
原发性活动性感染性心内膜炎的二尖瓣修复术在技术上具有挑战性。与瓣膜置换相比,其生存获益尚未明确确立,且由于修复失败和再次手术的高风险,可能并不存在生存获益。在本研究中,我们探讨了针对这些患者的结构化治疗方法的结果。
2000年1月至2017年1月期间,149例患者接受了原发性二尖瓣感染性心内膜炎的手术治疗。其中,97例(66%)患者接受了瓣膜修复,52例(34%)患者接受了瓣膜置换。我们的结构化治疗方法包括早期手术、彻底切除感染组织、广泛使用人工材料和“补片”修复技术。术中对预期修复的耐久性进行了严格评估,如果存在对长期耐久性的担忧,则不进行修复。为了研究瓣膜修复对总体生存的影响,进行了时间节点分析。
住院死亡率为15.4%(14例修复患者与9例置换患者;P = 0.642)。没有残留感染性心内膜炎病例或早期再次手术。在Cox比例风险分析中,瓣膜置换在术后1年内并不劣于修复[风险比(HR)1.134,95%置信区间(CI)0.504 - 2.540;P = 0.76]。术后1年以上,置换与生存率降低相关(HR 2.534,95% CI 1.002 - 6.406;P = 0.049)。在无复发性感染性心内膜炎(P = 0.47)和二尖瓣再次干预(P = 0.52)方面没有差异。
活动性二尖瓣心内膜炎仍然是一种复杂的疾病,具有显著的早期和晚期发病率和死亡率。结构化治疗方法使三分之二的患者能够接受瓣膜修复。通过关注早期手术,在瓣膜广泛破坏之前进行手术,以实现持久修复并改善晚期结局,临床结果可能会得到改善。