Department of Radiation Oncology, Taussig Cancer Center, Cleveland Clinic, Cleveland, OH, USA.
J Appl Clin Med Phys. 2020 Jul;21(7):77-83. doi: 10.1002/acm2.12887. Epub 2020 Apr 26.
To investigate the impact of breath-hold reproducibility on liver motion using a respiratory motion management device.
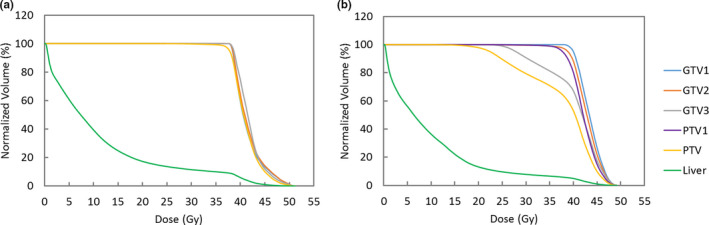
Forty-four patients with hepatic tumors, treated with SBRT with breath-hold, were randomly selected for this study. All patients underwent three consecutive computed tomography (CT) scans using active breath-hold coordinator (ABC) with three repeated single breath-hold during simulation. The three CT scans were labeled as ABC1-CT, ABC2-CT, and ABC3-CT. Displacements of centroids of the entire livers among the three ABC-CTs were measured as a surrogate for intrafractional motion. For each patient, two different treatment plans were prepared: (a) a clinical plan using a 5-mm expansion of an ITV that encompassed all three GTVs from each of the three ABC-CTs, and (b) a research plan using a 5-mm expansion of the GTV from only ABC1-CT to create PTV. The clinical plan acceptance criteria were that 95% of the PTV and 99% of the GTV received 100% of the prescription dose. Dosimetric endpoints were analyzed and compared for the two plans.
All shifts in the medial-lateral direction (range: -3.9 to 2.0 mm) were within 5 mm while 7% of shifts in the anterior-posterior direction (range: -10.5 to 16.7 mm) and 11% of shifts in the superior-inferior direction (range: -17.0 to 8.7 mm) exceeded 5 mm. Six patients (14%) had an intrafraction motion greater than 5 mm in any direction. For these six patients, if a plan was created based on a PTV from a single CT (ex. ABC1-CT), 5 of 12 GTVs captured from other ABC-CTs would fail to meet the clinical acceptance criteria due to poor breath-hold reproducibility.
Non-negligible intrafractional motion occurs in patients with poor breath-hold reproducibility. To identify this subgroup of patients, acquiring three CTs with active breath-hold during simulation is a feasible practical method.
使用呼吸运动管理设备研究呼吸可重复性对肝脏运动的影响。
本研究随机选择 44 例接受 SBRT 并进行屏气治疗的肝肿瘤患者。所有患者在模拟过程中使用主动屏气协调器(ABC)进行了三次连续的 CT 扫描,每次扫描重复进行三次单屏气。这三次 CT 扫描分别标记为 ABC1-CT、ABC2-CT 和 ABC3-CT。通过测量三次 ABC-CT 中肝脏中心点的位移来替代分次内运动。对于每位患者,分别制定了两种不同的治疗计划:(a)使用包含三个 ABC-CT 中所有三个 GTV 的 ITV 外扩 5mm 的临床计划;(b)使用仅 ABC1-CT 的 GTV 外扩 5mm 来创建 PTV 的研究计划。临床计划的接受标准是,95%的 PTV 和 99%的 GTV 接受 100%的处方剂量。分析并比较了两种计划的剂量学终点。
所有在中-侧方向的移动(范围:-3.9 至 2.0mm)都在 5mm 以内,而 7%的前-后方向的移动(范围:-10.5 至 16.7mm)和 11%的上-下方向的移动(范围:-17.0 至 8.7mm)超过了 5mm。有 6 名患者(14%)在任何方向的分次内运动都超过了 5mm。对于这 6 名患者,如果根据单次 CT(例如 ABC1-CT)创建计划,则由于呼吸可重复性差,12 个 GTV 中有 5 个无法满足临床接受标准。
在呼吸可重复性差的患者中会发生不可忽略的分次内运动。为了识别出这部分患者,在模拟过程中获取三次带主动屏气的 CT 扫描是一种可行的实用方法。