Department of Urology, Emory University School of Medicine, Atlanta, Georgia.
Department of Radiology and Imaging Sciences, Emory University School of Medicine, Atlanta, Georgia.
J Urol. 2020 Oct;204(4):734-740. doi: 10.1097/JU.0000000000001095. Epub 2020 Apr 29.
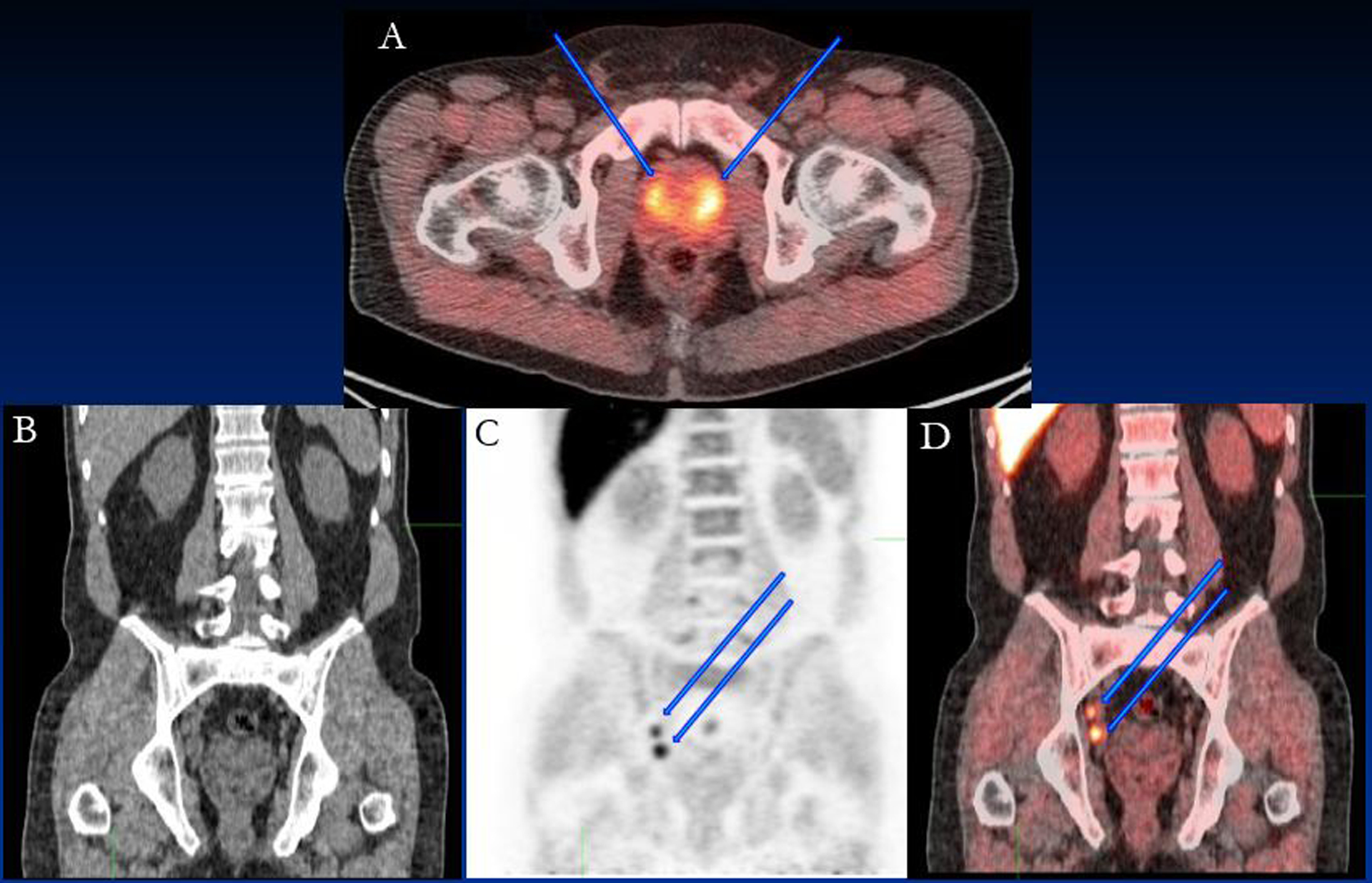
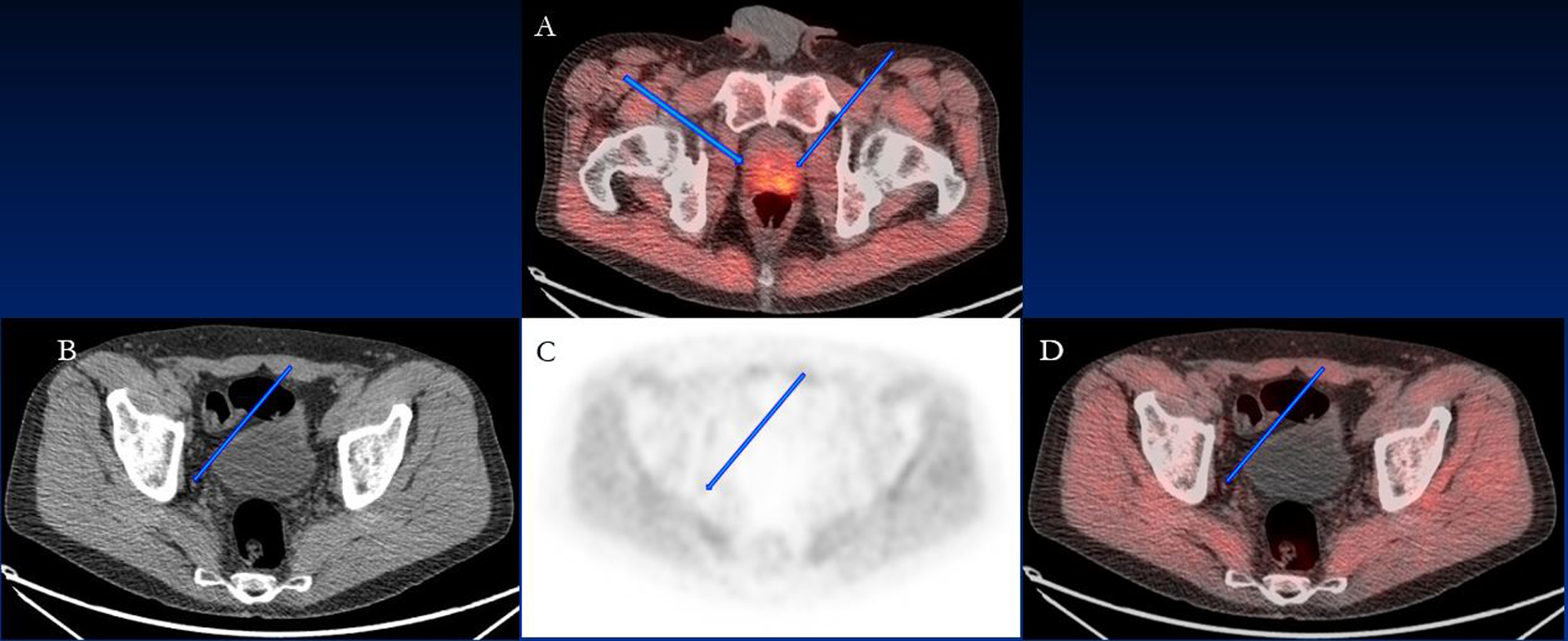
Accurate preoperative staging of prostate cancer is essential for treatment planning. Conventional imaging is limited in detection of metastases. Our primary aim was to determine if [F]fluciclovine positron emission tomography/computerized tomography is an early indicator of subclinical metastasis among patients with high risk prostate cancer.
A total of 68 patients with unfavorable intermediate to very high risk prostate cancer without systemic disease on conventional imaging were recruited before robotic radical prostatectomy with extended pelvic lymph node dissection. Diagnostic performance of [F]fluciclovine positron emission tomography/computerized tomography and conventional imaging for detection of metastatic disease, and correlation of positivity to node and metastatic deposit size were determined.
Overall 57 of 68 patients completed the protocol, of whom 31 had nodal metastasis on histology. [F]Fluciclovine positron emission tomography/computerized tomography sensitivity and specificity in detecting nodal metastasis was 55.3% and 84.8% per patient, and 54.8% and 96.4% per region (right and left pelvis, presacral and nonregional), respectively. Compared with conventional imaging [F]Fluciclovine positron emission tomography/computerized tomography had significantly higher sensitivity on patient based (55.3% vs 33.3%, p <0.01) and region based (54.8% vs 19.4%, p <0.01) analysis, detecting metastasis in 7 more patients and 22 more regions, with similar high specificity. Four additional patients had distant disease or other cancer detected on [F] fluciclovine positron emission tomography/computerized tomography which precluded surgery. Detection of metastasis was related to size of metastatic deposits within lymph nodes and overall metastatic burden.
[F]Fluciclovine positron emission tomography/computerized tomography detects occult metastases not identified on conventional imaging and may help guide treatment decisions and lymph node dissection due to high specificity for metastatic disease.
准确的前列腺癌术前分期对于治疗计划至关重要。常规影像学检查在检测转移方面存在局限性。我们的主要目的是确定[F]氟尿苷正电子发射断层扫描/计算机断层扫描是否是高危前列腺癌患者亚临床转移的早期指标。
共招募了 68 名无系统性疾病的不利中间至极高危前列腺癌患者,这些患者在接受机器人根治性前列腺切除术和广泛盆腔淋巴结清扫术之前接受了[F]氟尿苷正电子发射断层扫描/计算机断层扫描检查。确定[F]氟尿苷正电子发射断层扫描/计算机断层扫描和常规影像学检查对检测转移性疾病的诊断性能,以及阳性与淋巴结和转移灶大小的相关性。
共有 68 名患者中的 57 名完成了该方案,其中 31 名患者的组织学上存在淋巴结转移。[F]氟尿苷正电子发射断层扫描/计算机断层扫描检测淋巴结转移的敏感性和特异性分别为 55.3%和 84.8%/患者,54.8%和 96.4%/区域(右和左骨盆、骶前和非区域)。与常规影像学检查相比,[F]氟尿苷正电子发射断层扫描/计算机断层扫描在患者(55.3%比 33.3%,p<0.01)和区域(54.8%比 19.4%,p<0.01)分析中具有更高的敏感性,分别检测到 7 例和 22 例更多的转移病例,特异性也很高。另外 4 名患者在[F]氟尿苷正电子发射断层扫描/计算机断层扫描中发现远处疾病或其他癌症,从而无法进行手术。转移的检测与淋巴结内转移灶的大小和总体转移负担有关。
[F]氟尿苷正电子发射断层扫描/计算机断层扫描可检测到常规影像学检查未发现的隐匿性转移,由于对转移性疾病具有很高的特异性,因此可能有助于指导治疗决策和淋巴结清扫。