Department of Radiation Oncology, Winship Cancer Institute, Emory University, Atlanta, Georgia.
Biostatistics and Bioinformatics Shared Resource, Winship Cancer Institute, Emory University, Atlanta, Georgia.
JAMA Netw Open. 2020 Dec 1;3(12):e2025143. doi: 10.1001/jamanetworkopen.2020.25143.
Long-term control of node-positive (N1) prostate cancer, the incidence of which is increasing, is obtainable with aggressive treatment, and definitive external beam radiation therapy (EBRT) with long-term androgen deprivation therapy (ADT) is an increasingly preferred option. Caring for these patients is complex and may require resources more readily available at high-volume centers.
To evaluate the association between radiation facility case volume and overall survival (OS) in men with N1 prostate cancer.
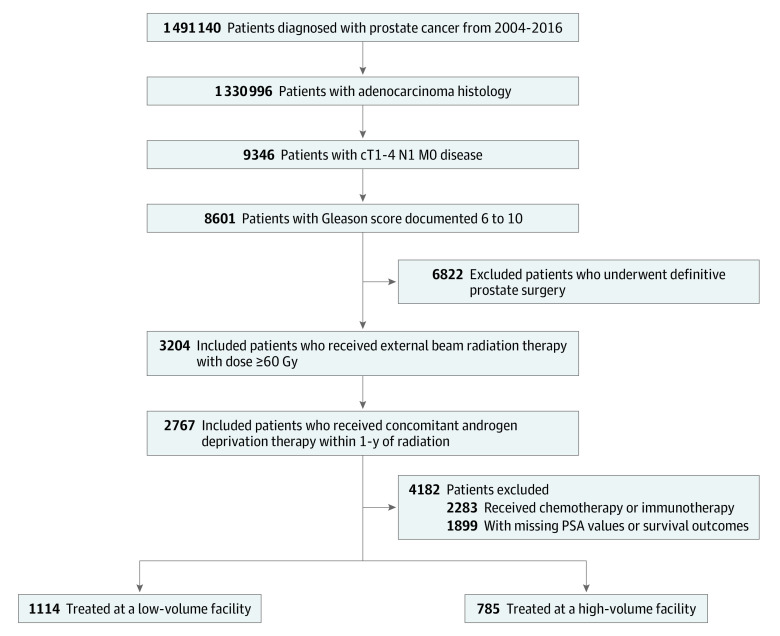
DESIGN, SETTING, AND PARTICIPANTS: This cohort study included 1899 men diagnosed with T1N1M0 to T4N1M0 prostate cancer treated with curative-intent EBRT and ADT between January 2004 and December 2016 at US facilities reporting to the National Cancer Database. Data analysis was performed from March to June 2020.
Treatment at a center with high vs low average cumulative facility volume (ACFV), defined as the total number of prostate radiation cases at an individual patient's treatment facility from 2004 until the year of that patient's diagnosis.
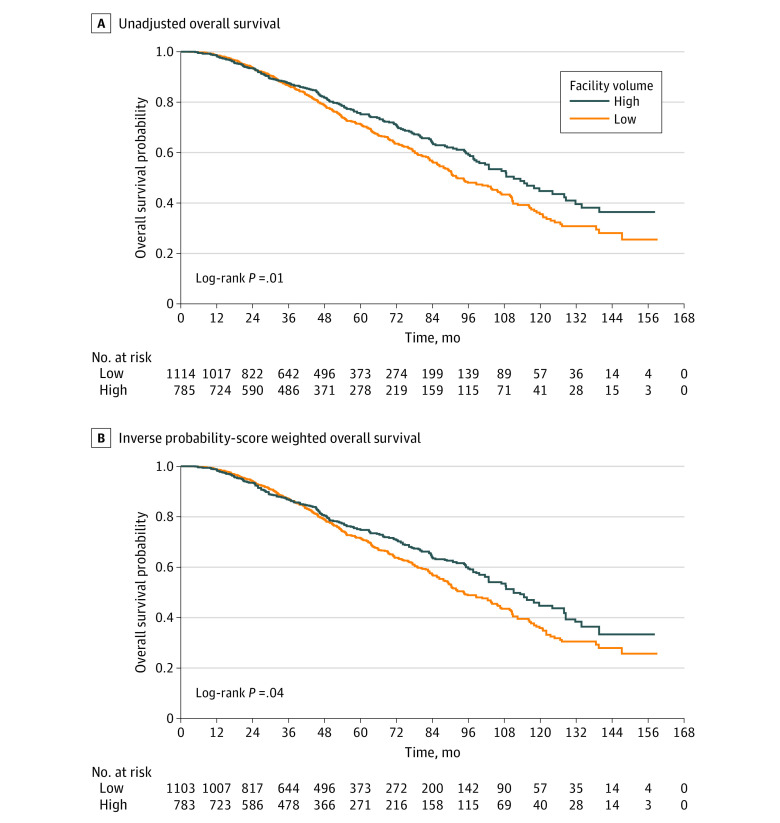
OS was assessed between high- vs low-ACFV centers using the Kaplan-Meier method with and without propensity score-based weighted adjustment and multivariable Cox proportional hazards. The nonlinear association between continuous ACFV and OS was examined through a Martingale residual plot, and the optimal ACFV cutoff point that maximized the separation between high vs low ACFV was identified via a bias adjusted log rank test.
A total of 1899 men met inclusion criteria. The median (interquartile range) age was 66 (60-72) years, 1491 (78.5%) were White individuals, and 1145 (60.3%) were treated at nonacademic centers. The optimal ACFV cutoff point was 66.4 patients treated per year. The median OS for patients treated at high-ACFV vs low-ACFV centers was 111.1 (95% CI, 101.5-127.9) months and 92.3 (95% CI, 87.7-103.9) months, respectively (P = .01). On multivariable analysis, treatment at a low-ACFV center was associated with increased risk of death (HR, 1.22; 95% CI, 1.02-1.46, P = .03) compared with treatment at a high-ACFV center. These results persisted after propensity score-based adjustment.
This cohort study found a significant association of facility case volume with long-term outcomes in men with N1 prostate cancer undergoing EBRT with ADT. Specifically, treatment at a facility with high radiation case volume was independently associated with longer OS. Further studies should focus on identifying which factors unique to high-volume centers may be responsible for this benefit.
随着 N1 期前列腺癌发病率的增加,这种疾病可以通过积极治疗得到长期控制,并且越来越多的人选择采用外照射放射治疗(EBRT)联合长期雄激素剥夺治疗(ADT)作为确定性治疗方法。治疗这些患者情况复杂,可能需要在高容量中心才能获得的资源。
评估前列腺癌 N1 期患者的放射治疗设施病例数量与总生存(OS)之间的关系。
设计、地点和参与者:本队列研究纳入了 2004 年 1 月至 2016 年 12 月期间在美国国家癌症数据库报告的设施中接受根治性 EBRT 和 ADT 治疗的 1899 例 T1N1M0 至 T4N1M0 前列腺癌患者。数据分析于 2020 年 3 月至 6 月进行。
在高(与低)平均累积设施量(ACFV)中心治疗,定义为从 2004 年到患者诊断当年每位患者在治疗设施的前列腺放射治疗病例总数。
使用 Kaplan-Meier 方法评估高 ACFV 与低 ACFV 中心之间的 OS,并进行倾向评分加权调整和多变量 Cox 比例风险分析。通过 Martingale 残差图检查连续 ACFV 与 OS 之间的非线性关系,并通过偏置调整对数秩检验确定最大程度区分高 ACFV 与低 ACFV 的最佳 ACFV 截止值。
共纳入 1899 例患者。中位(四分位间距)年龄为 66(60-72)岁,1491 例(78.5%)为白人,1145 例(60.3%)在非学术中心接受治疗。最佳 ACFV 截止值为每年治疗 66.4 例患者。在高 ACFV 与低 ACFV 中心治疗的患者中位 OS 分别为 111.1(95%CI,101.5-127.9)个月和 92.3(95%CI,87.7-103.9)个月(P=0.01)。多变量分析显示,与高 ACFV 中心相比,低 ACFV 中心治疗与死亡风险增加相关(HR,1.22;95%CI,1.02-1.46,P=0.03)。这些结果在基于倾向评分的调整后仍然存在。
本队列研究发现,设施病例数量与接受 EBRT 联合 ADT 治疗的 N1 期前列腺癌患者的长期结局显著相关。具体来说,在高放射治疗病例量的机构接受治疗与更长的 OS 独立相关。进一步的研究应集中于确定高容量中心的哪些特有因素可能是这种获益的原因。