Department of Palliative Care, Policy and Rehabilitation, Faculty of Life Sciences & Medicine, Cicely Saunders Institute, King's College London, London, UK.
Faculty of Life Sciences & Medicine, School of Division of Primary Care & Public Health Sciences, King's College London, London, UK.
BMC Fam Pract. 2020 Apr 29;21(1):76. doi: 10.1186/s12875-020-01127-8.
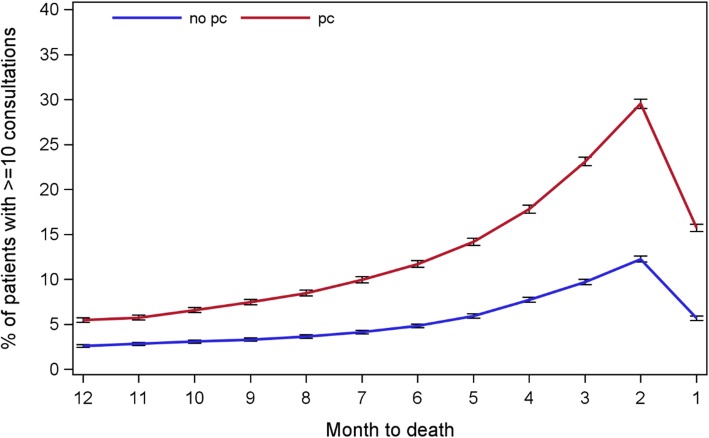
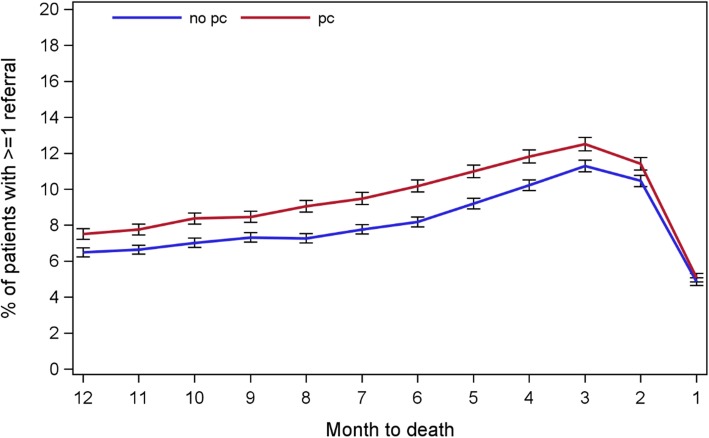
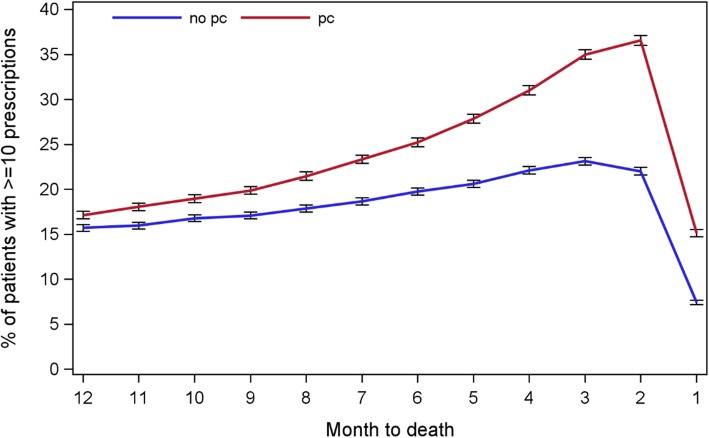
End of life (EoL) care becomes more complex and increasingly takes place in the community, but there is little data on the use of general practice (GP) services to guide care improvement. This study aims to determine the trends and factors associated with GP consultation, prescribing and referral to other care services amongst cancer patients in the last year of life.
A retrospective cohort study of cancer patients who died in 2000-2014, based on routinely collected primary care data (the Clinical Practice Research DataLink, CPRD) covering a representative sample of the population in the United Kingdom. Outcome variables were number of GP consultations (primary), number of prescriptions and referral to other care services (yes vs no) in the last year of life. Explanatory variables included socio-demographics, clinical characteristics and the status of palliative care needs recognised or not. The association between outcome and explanatory variables were evaluated using multiple-adjusted risk ratio (aRR).
Of 68,523 terminal cancer patients, 70% were aged 70+, 75% had comorbidities and 45.5% had palliative care needs recognised. In the last year of life, a typical cancer patient had 43 GP consultations (Standard deviation (SD): 31.7; total = 3,031,734), 71.5 prescriptions (SD: 68.0; total = 5,074,178), and 21(SD: 13.0) different drugs; 58.0% of patients had at least one referral covering all main clinical specialities. More comorbid conditions, prostate cancer and having palliative care needs recognised were associated with more primary care consultations, more prescriptions and a higher chance of referral (aRRs 1.07-2.03). Increasing age was related to fewer consultations (aRRs 0.77-0.96), less prescriptions (aRR 1.09-1.44), and a higher chance of referral (aRRs 1.08-1.16) but less likely to have palliative care needs recognised (aRRs 0.53-0.89).
GPs are very involved in end of life care of cancer patients, most of whom having complex care needs, i.e. older age, comorbidity and polypharmacy. This highlights the importance of enhancing primary palliative care skills among GPs and the imperative of greater integration of primary care with other healthcare professionals including oncologists, palliative care specialists, geriatricians and pharmacists. Research into the potential of deprescribing is warranted. Older patients have poorer access to both primary care and palliative care need to be addressed in future practices.
临终关怀变得更加复杂,越来越多的临终关怀发生在社区中,但几乎没有关于使用全科医生(GP)服务来指导护理改进的数据。本研究旨在确定癌症患者在生命的最后一年中 GP 咨询、处方和转介到其他护理服务的趋势和相关因素。
这是一项基于常规收集的初级保健数据(临床实践研究数据链接,CPRD)的回顾性队列研究,该数据涵盖了英国代表性人群的样本。结局变量为生命最后一年的 GP 咨询次数(初级)、处方数量和转介到其他护理服务(是/否)。解释变量包括社会人口统计学特征、临床特征以及是否认识到姑息治疗需求。使用多调整风险比(aRR)评估结局与解释变量之间的关联。
在 68523 名晚期癌症患者中,70%的患者年龄在 70 岁以上,75%的患者合并症,45.5%的患者有姑息治疗需求。在生命的最后一年,典型的癌症患者有 43 次 GP 咨询(标准差(SD):31.7;总数=3031734),71.5 次处方(SD:68.0;总数=5074178)和 21 种不同的药物;58.0%的患者至少有一次涵盖所有主要临床专业的转介。更多的合并症、前列腺癌和姑息治疗需求的认识与更多的初级保健咨询、更多的处方和更高的转诊机会相关(aRRs 1.07-2.03)。年龄的增加与咨询次数减少(aRRs 0.77-0.96)、处方减少(aRR 1.09-1.44)和转诊机会增加(aRRs 1.08-1.16)相关,但姑息治疗需求的认识减少(aRRs 0.53-0.89)。
GP 非常参与癌症患者的临终关怀,其中大多数患者有复杂的护理需求,即年龄较大、合并症和多药治疗。这凸显了提高 GP 初级姑息治疗技能的重要性,以及加强初级保健与包括肿瘤学家、姑息治疗专家、老年病学家和药剂师在内的其他医疗保健专业人员之间整合的必要性。有必要研究减少处方的潜力。在未来的实践中,需要解决老年患者在初级保健和姑息治疗需求方面的较差获得情况。