Department of Laboratory Medicine, Karolinska Institutet, Stockholm, Sweden.
Department of Medicine, Karolinska Institutet, Stockholm, Sweden.
J Virol. 2020 Jul 1;94(14). doi: 10.1128/JVI.02128-19.
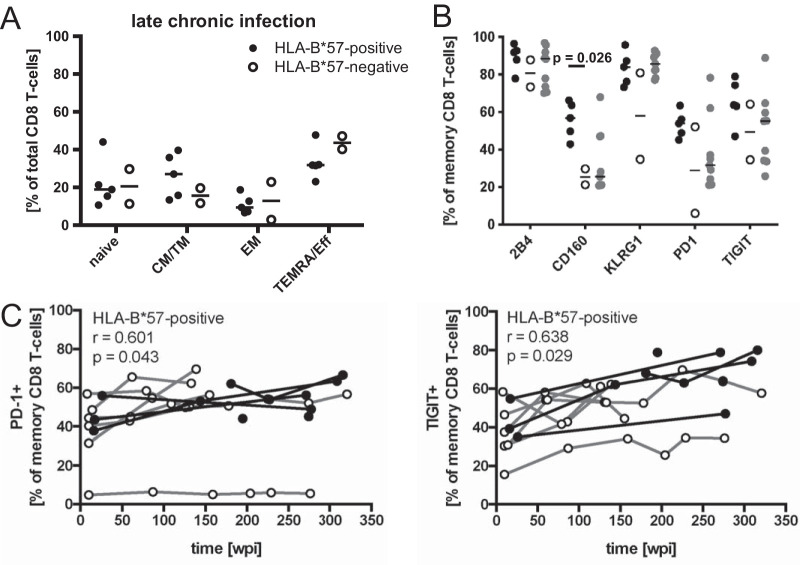
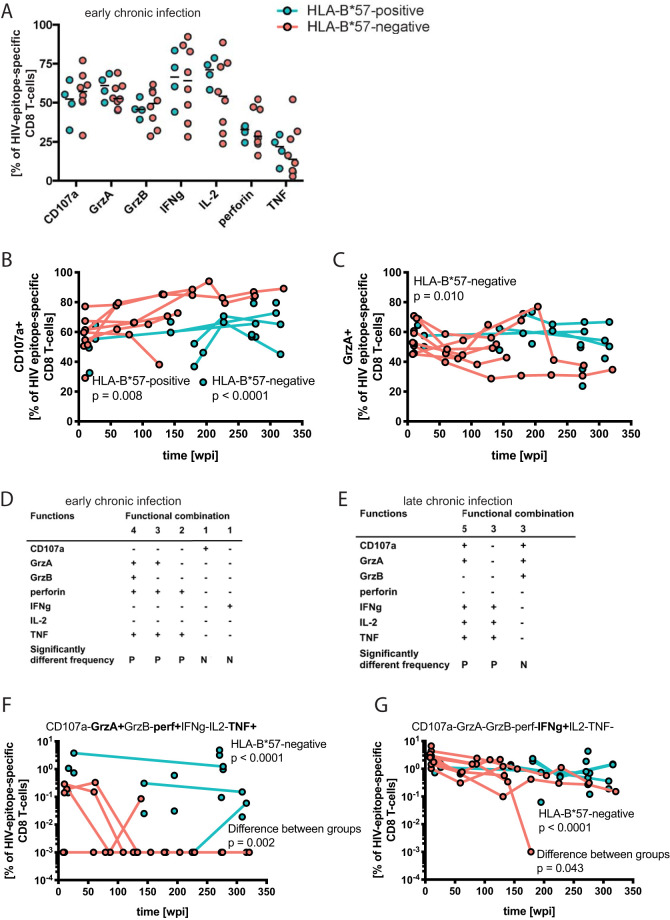
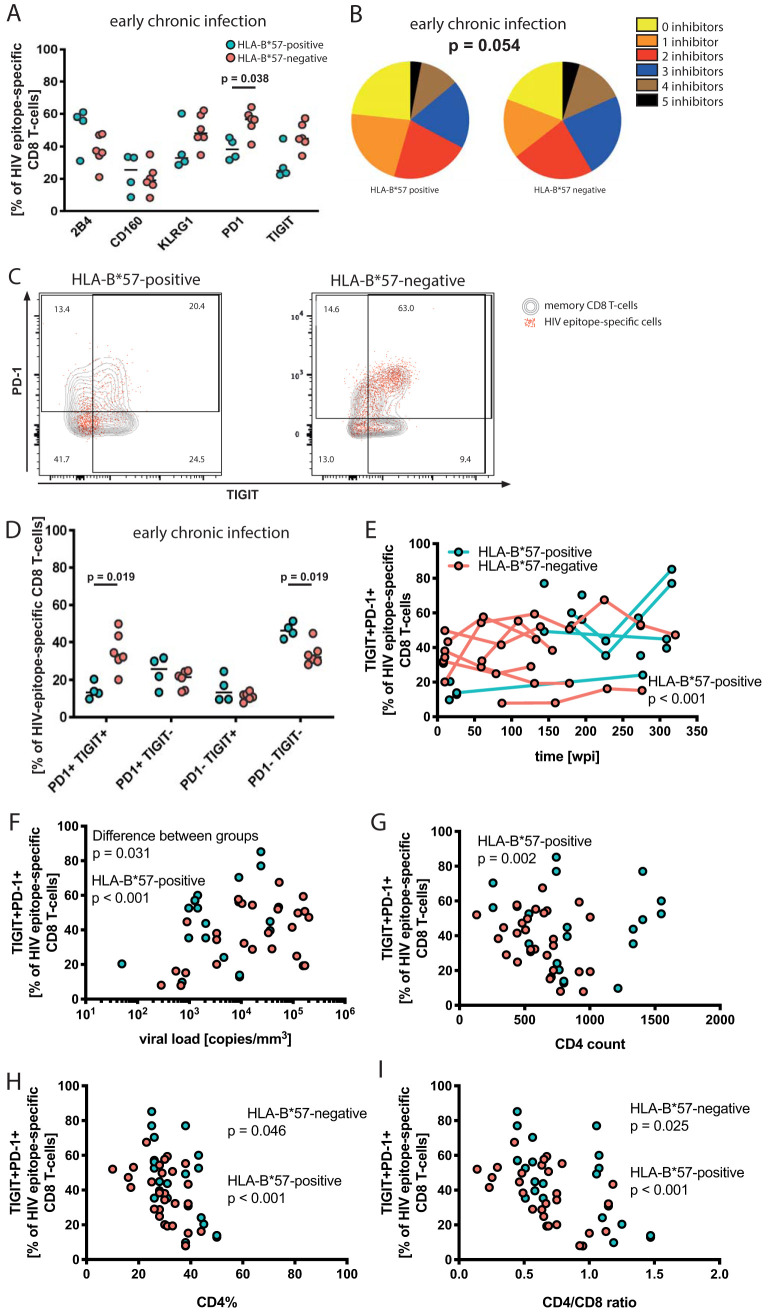
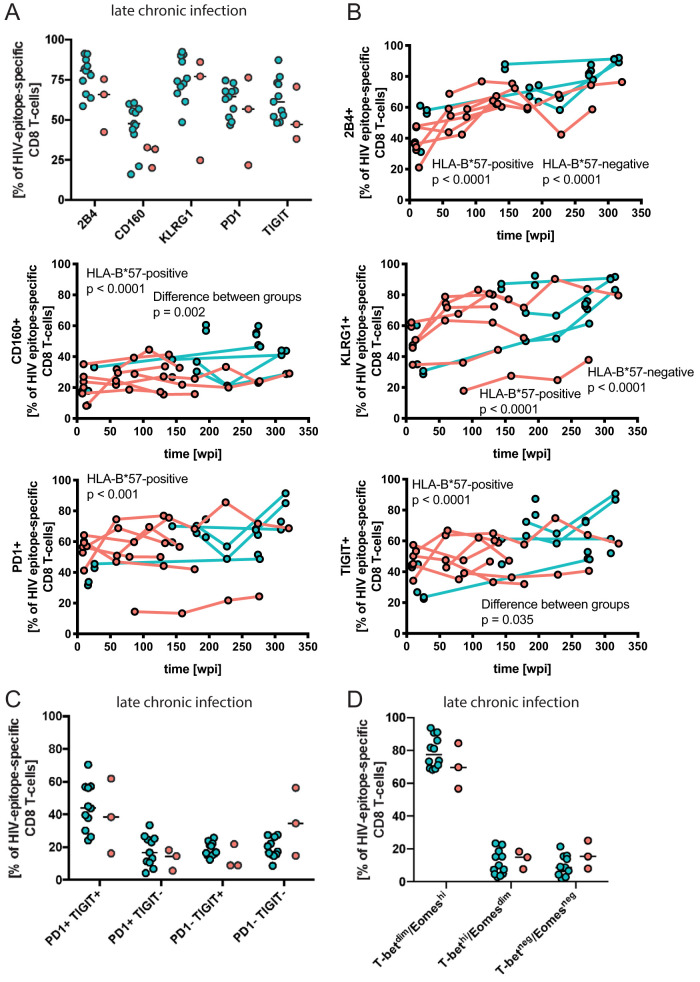
While the relationship of protective human leukocyte antigen (HLA) class I alleles and HIV progression is well defined, the interaction of HLA-mediated protection and CD8 T-cell exhaustion is less well characterized. To gain insight into the influence of HLA-B57:01 on the deterioration of CD8 T-cell responses during HIV infection in the absence of antiretroviral treatment, we compared HLA-B57:01-restricted HIV-specific CD8 T-cell responses to responses restricted by other HLA class I alleles longitudinally after control of peak viremia. Detailed characterization of polyfunctionality, differentiation phenotypes, transcription factor, and inhibitory receptor expression revealed progression of CD8 T-cell exhaustion over the course of the infection in both patient groups. However, early effects on the phenotype of the total CD8 T-cell population were apparent only in HLA-B57-negative patients. The HLA-B57:01-restricted, HIV epitope-specific CD8 T-cell responses showed beneficial functional patterns and significantly lower frequencies of inhibitory receptor expression, i.e., PD-1 and coexpression of PD-1 and TIGIT, within the first year of infection. Coexpression of PD-1 and TIGIT was correlated with clinical markers of disease progression and declining percentages of the T-bet Eomes CD8 T-cell population. In accordance with clinical and immunological deterioration in the HLA-B*57:01 group, the difference in PD-1 and TIGIT receptor expression did not persist to later stages of the disease. Given the synergistic nature of TIGIT and PD-1, the coexpression of those inhibitory receptors should be considered when evaluating T-cell pathogenesis, developing immunomodulatory therapies or vaccines for HIV, and when using immunotherapy or vaccination for other causes in HIV-infected patients. HIV-mediated T-cell exhaustion influences the patient´s disease progression, immune system and subsequently non-AIDS complications, and efficacy of vaccinations against other pathogens. Consequently, the possibilities of interfering with exhaustion are numerous. Expanding the use of immunomodulatory therapies to include HIV treatment depends on information about possible targets and their role in the deterioration of the immune system. Furthermore, the rise of immunotherapies against cancer and elevated cancer incidence in HIV-infected patients together increase the need for detailed knowledge of T-cell exhaustion and possible interactions. A broader approach to counteract immune exhaustion to alleviate complications and improve efficacy of other vaccines also promises to increase patients' health and quality of life.
虽然保护性人类白细胞抗原(HLA)I 类等位基因与 HIV 进展之间的关系已经得到很好的定义,但 HLA 介导的保护作用与 CD8 T 细胞耗竭之间的相互作用还不太清楚。为了深入了解在没有抗逆转录病毒治疗的情况下,HLA-B57:01 对 HIV 感染期间 CD8 T 细胞反应恶化的影响,我们比较了 HLA-B57:01 限制的 HIV 特异性 CD8 T 细胞反应与其他 HLA I 类等位基因限制的反应,这些反应是在控制峰值病毒血症后纵向进行的。详细的多能性、分化表型、转录因子和抑制性受体表达特征表明,在两组患者中,随着感染的进展,CD8 T 细胞耗竭都在进展。然而,在 HLA-B57 阴性患者中,仅在感染早期对总 CD8 T 细胞群体的表型有明显影响。在感染的第一年,HLA-B57:01 限制的 HIV 表位特异性 CD8 T 细胞反应表现出有益的功能模式,并且抑制性受体表达的频率显著降低,即 PD-1 和 PD-1 与 TIGIT 的共表达。PD-1 和 TIGIT 的共表达与疾病进展的临床标志物以及 T-bet Eomes CD8 T 细胞群体的百分比下降相关。与 HLA-B*57:01 组的临床和免疫恶化一致,这些抑制性受体的表达差异在疾病的后期阶段并未持续存在。鉴于 TIGIT 和 PD-1 的协同性质,在评估 T 细胞发病机制、开发针对 HIV 的免疫调节疗法或疫苗以及在 HIV 感染患者中使用免疫疗法或疫苗治疗其他原因时,应考虑这些抑制性受体的共表达。HIV 介导的 T 细胞耗竭会影响患者的疾病进展、免疫系统,进而影响非艾滋病并发症以及针对其他病原体的疫苗的效果。因此,干预耗竭的可能性很多。将免疫调节疗法的应用扩展到包括 HIV 治疗取决于有关可能靶点及其在免疫系统恶化中的作用的信息。此外,针对癌症的免疫疗法的兴起以及 HIV 感染患者中癌症发病率的升高,都增加了对 T 细胞耗竭及其可能相互作用的详细了解的需求。采取更广泛的方法来对抗免疫衰竭,以减轻并发症并提高其他疫苗的效果,也有望提高患者的健康和生活质量。