The George Institute for Global Health, University of New South Wales Sydney, Sydney, New South Wales, Australia
Concord Repatriation General Hospital, Sydney, New South Wales, Australia.
J Am Soc Nephrol. 2020 May;31(5):1128-1139. doi: 10.1681/ASN.2019111168.
Canagliflozin reduced renal and cardiovascular events in people with type 2 diabetes in the CREDENCE trial. We assessed efficacy and safety of canagliflozin by initial estimated glomerular filtration rate (eGFR).
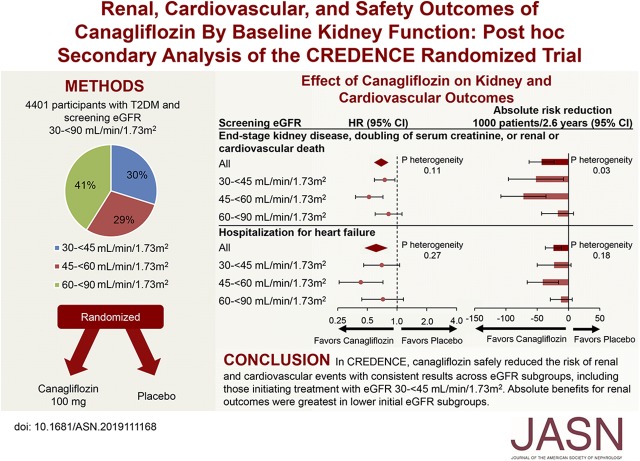
CREDENCE randomly assigned 4401 participants with an eGFR of 30 to <90 ml/min per 1.73 m and substantial albuminuria to canagliflozin 100 mg or placebo. We used Cox proportional hazards regression to analyze effects on renal and cardiovascular efficacy and safety outcomes within screening eGFR subgroups (30 to <45, 45 to <60, and 60 to <90 ml/min per 1.73 m) and linear mixed effects models to analyze the effects on eGFR slope.
At screening, 1313 (30%), 1279 (29%), and 1809 (41%) participants had an eGFR of 30 to <45, 45 to <60, and 60 to <90 ml/min per 1.73 m, respectively. The relative benefits of canagliflozin for renal and cardiovascular outcomes appeared consistent among eGFR subgroups (all interaction >0.11). Subgroups with lower eGFRs, who were at greater risk, exhibited larger absolute benefits for renal outcomes. Canagliflozin's lack of effect on serious adverse events, amputations, and fractures appeared consistent among eGFR subgroups. In all subgroups, canagliflozin use led to an acute eGFR drop followed by relative stabilization of eGFR loss. Among those with an eGFR of 30 to <45 ml/min per 1.73 m, canagliflozin led to an initial drop of 2.03 ml/min per 1.73 m. Thereafter, decline in eGFR was slower in the canagliflozin versus placebo group (-1.72 versus -4.33 ml/min per 1.73 m; between-group difference 2.61 ml/min per 1.73 m).
Canagliflozin safely reduced the risk of renal and cardiovascular events, with consistent results across eGFR subgroups, including the subgroup initiating treatment with an eGFR of 30 to <45 ml/min per 1.73 m. Absolute benefits for renal outcomes were greatest in subgroups with lower eGFR.
Evaluation of the Effects of Canagliflozin on Renal and Cardiovascular Outcomes in Participants With Diabetic Nephropathy (CREDENCE), NCT02065791.
卡格列净可降低 2 型糖尿病患者的肾脏和心血管事件。我们根据初始估算肾小球滤过率(eGFR)评估卡格列净的疗效和安全性。
CREDENCE 试验将 eGFR 为 30 至<90 ml/min/1.73m 且大量蛋白尿的 4401 名参与者随机分为卡格列净 100mg 或安慰剂组。我们使用 Cox 比例风险回归分析在筛查 eGFR 亚组(30 至<45、45 至<60 和 60 至<90 ml/min/1.73m)内对肾脏和心血管疗效和安全性结局的影响,并使用线性混合效应模型分析对 eGFR 斜率的影响。
在筛查时,1313(30%)、1279(29%)和 1809(41%)名参与者的 eGFR 分别为 30 至<45、45 至<60 和 60 至<90 ml/min/1.73m。eGFR 亚组之间卡格列净对肾脏和心血管结局的相对益处似乎一致(所有交互作用>0.11)。eGFR 较低、风险较高的亚组,肾脏结局的绝对获益更大。eGFR 亚组之间卡格列净对严重不良事件、截肢和骨折的影响似乎一致。在所有亚组中,卡格列净的使用导致 eGFR 急性下降,随后 eGFR 丢失相对稳定。在 eGFR 为 30 至<45 ml/min/1.73m 的亚组中,卡格列净导致初始 eGFR 下降 2.03 ml/min/1.73m。此后,卡格列净组的 eGFR 下降速度比安慰剂组慢(-1.72 与-4.33 ml/min/1.73m;组间差异 2.61 ml/min/1.73m)。
卡格列净可安全降低肾脏和心血管事件风险,eGFR 亚组结果一致,包括 eGFR 为 30 至<45 ml/min/1.73m 开始治疗的亚组。eGFR 较低的亚组肾脏结局的绝对获益最大。
评估卡格列净对糖尿病肾病患者肾脏和心血管结局影响的试验(CREDENCE),NCT02065791。