Zannad Faiez, McGuire Darren K, Ortiz Alberto
Inserm, Centre d'Investigation Clinique Plurithématique 1433, U1116, CHRU de Nancy, F-CRIN INI-CRCT Université de Lorraine, Nancy, France.
Division of Cardiology, Department of Internal Medicine, The University of Texas Southwestern Medical Center and Parkland Health, Dallas, USA.
J Intern Med. 2025 May;297(5):460-478. doi: 10.1111/joim.20050. Epub 2024 Dec 31.
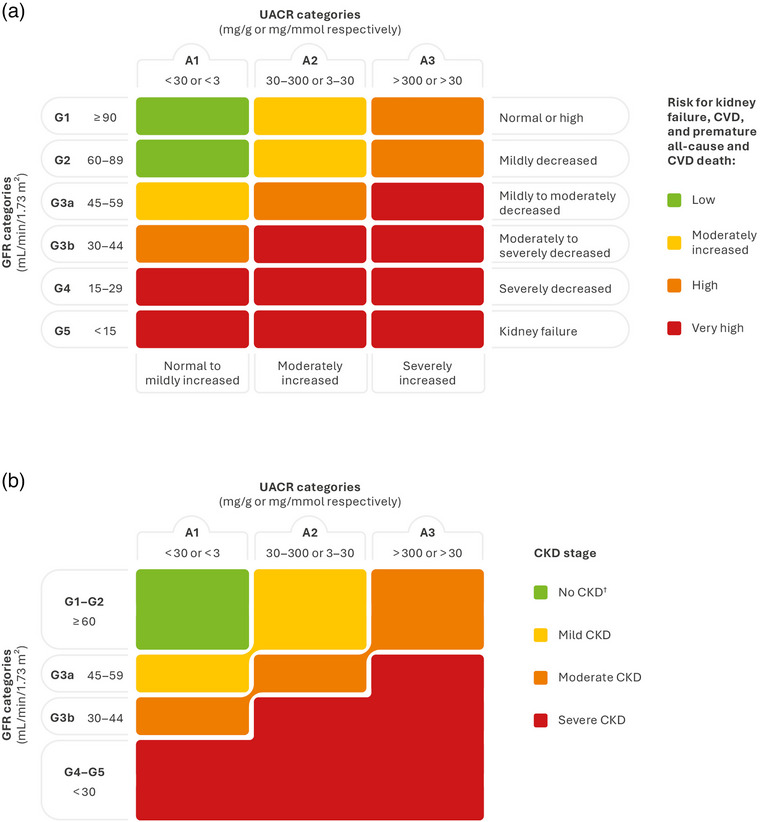
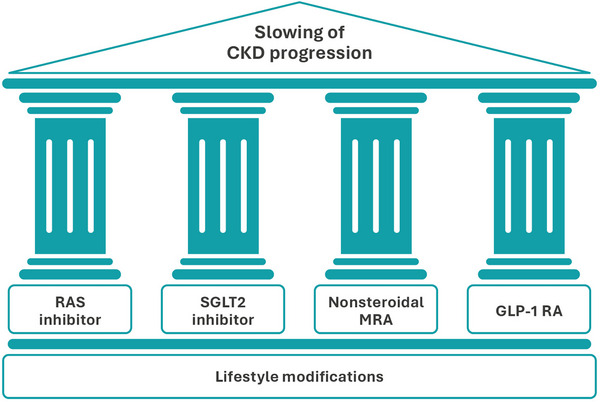
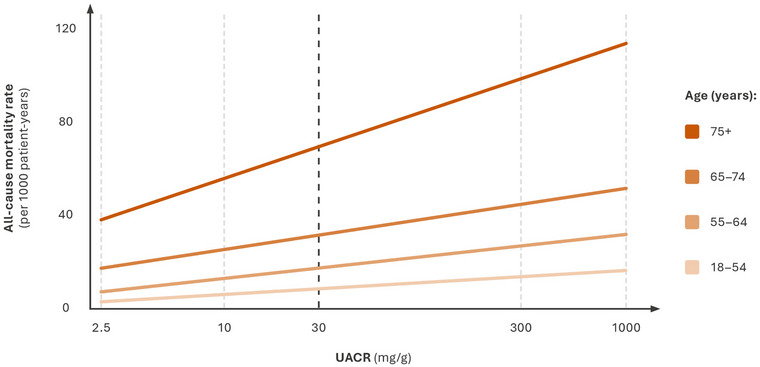
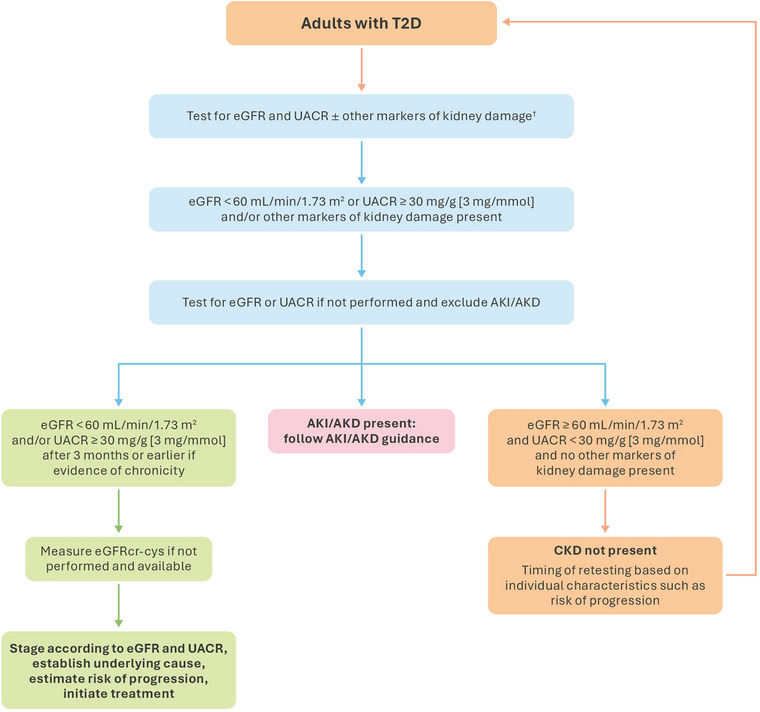
Chronic kidney disease (CKD) is a prevalent and progressive condition associated with significant mortality and morbidity. Diabetes is a common cause of CKD, and both diabetes and CKD increase the risk of cardiovascular disease (CVD), the leading cause of death in individuals with CKD. This review will discuss the importance of early detection of CKD and prompt pharmacological intervention to slow CKD progression and delay the development of CVD for improving outcomes. Early CKD is often asymptomatic, and diagnosis usually requires laboratory testing. The combination of estimated glomerular filtration rate (eGFR) and urine albumin-to-creatinine ratio (UACR) measurements is used to diagnose and determine CKD severity. Guidelines recommend at least annual screening for CKD in at-risk individuals. While eGFR testing rates are consistently high, rates of UACR testing remain low. This results in underdiagnosis and undertreatment of CKD, leaving many individuals at risk of CKD progression and CVD. UACR testing is an actionable component of the CKD definition. A four-pillar treatment approach for slowing the progression of diabetic kidney disease is suggested, comprising a renin-angiotensin-system (RAS) inhibitor, a sodium-glucose cotransporter 2 inhibitor, a glucagon-like peptide 1 receptor agonist, and the nonsteroidal mineralocorticoid receptor antagonist finerenone. The combination of these agents provides a greater cardiorenal risk reduction compared with RAS inhibitors alone. Early detection of CKD and prompt intervention with guideline-directed medical therapy are crucial for reducing CVD risk in individuals with CKD and diabetes. Evidence from ongoing studies will advance our understanding of optimal therapy in this population.
慢性肾脏病(CKD)是一种普遍且呈进行性发展的疾病,与显著的死亡率和发病率相关。糖尿病是CKD的常见病因,糖尿病和CKD都会增加心血管疾病(CVD)的风险,而CVD是CKD患者的主要死因。本综述将讨论早期检测CKD以及及时进行药物干预以减缓CKD进展和延缓CVD发生从而改善预后的重要性。早期CKD通常无症状,诊断通常需要实验室检测。估算肾小球滤过率(eGFR)和尿白蛋白与肌酐比值(UACR)测量结果相结合用于诊断和确定CKD的严重程度。指南建议对高危个体至少每年进行一次CKD筛查。虽然eGFR检测率一直很高,但UACR检测率仍然很低。这导致CKD的诊断不足和治疗不足,使许多人面临CKD进展和CVD的风险。UACR检测是CKD定义中一个可采取行动的组成部分。建议采用一种四支柱治疗方法来减缓糖尿病肾病的进展,包括肾素 - 血管紧张素系统(RAS)抑制剂、钠 - 葡萄糖协同转运蛋白2抑制剂、胰高血糖素样肽1受体激动剂和非甾体类盐皮质激素受体拮抗剂非奈利酮。与单独使用RAS抑制剂相比,这些药物联合使用可更大程度地降低心肾风险。早期检测CKD并及时采用指南指导的药物治疗对于降低CKD和糖尿病患者的CVD风险至关重要。正在进行的研究证据将增进我们对该人群最佳治疗方法的理解。