Gornet J-M, Tran Minh M L, Leleu F, Hassid D
Paris University, Department of Gastroenterology, AP-HP Hôpital Saint Louis, 1, avenue Claude Vellefaux, 75010 Paris, France.
Paris University, Department of Gastroenterology, AP-HP Hôpital Saint Louis, 1, avenue Claude Vellefaux, 75010 Paris, France.
J Visc Surg. 2020 Jun;157(3S1):S51-S57. doi: 10.1016/j.jviscsurg.2020.04.017. Epub 2020 Apr 24.
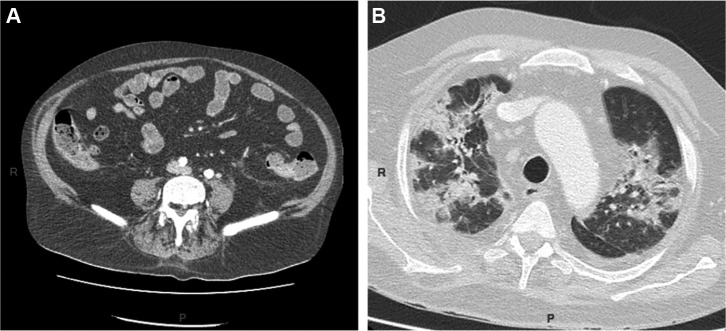
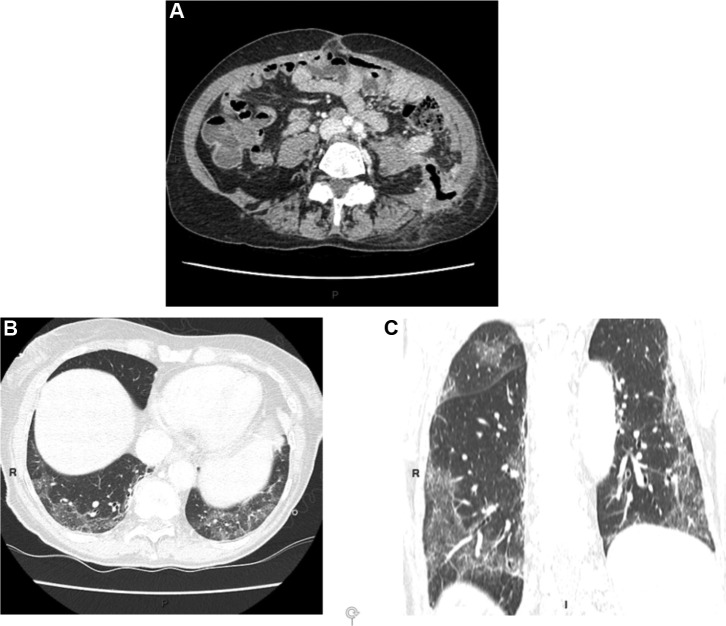
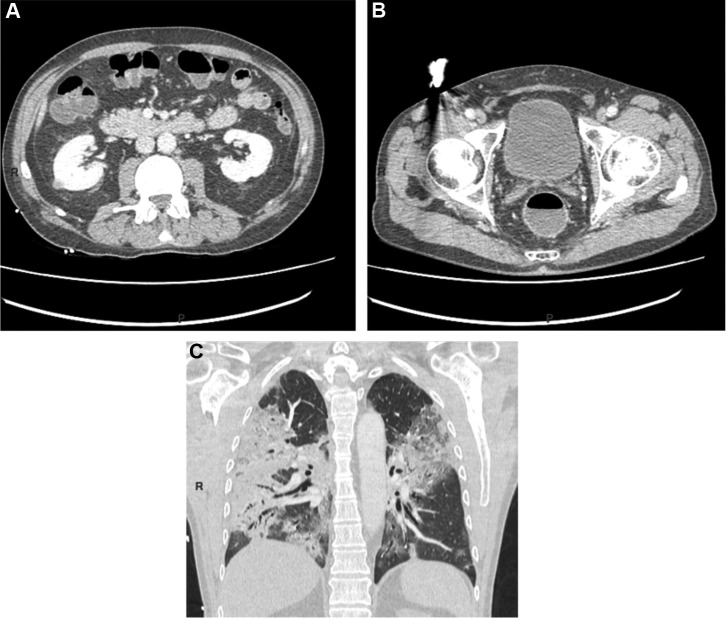
The symptoms associated with COVID-19 are mainly characterized by a triad composed of fever, dry cough and dyspnea. However, digestive symptoms have also been reported. At first considered as infrequent, they in fact seem to affect more than half of patients. The symptoms mainly include anorexia, diarrhea, nausea and/or vomiting and abdominal pain. Even though prognosis is associated with lung injury, digestive symptoms seem significantly more frequent in patients presenting with severe COVID-19 infection. Digestive presentations, which may be isolated or which can precede pulmonary symptoms, have indeed been reported, with diarrhea as a leading clinical sign. The main biological abnormalities that can suggest COVID-19 infection at an early stage are lymphopenia, elevated CRP and heightened ASAT transaminases. Thoraco-abdominal scan seems useful as a means of on the one hand ruling out digestive pathology not connected with coronavirus and on the other hand searching for pulmonary images consistent with COVID-19 infection. No data exist on the value of digestive endoscopy in cases of persistent digestive symptoms. Moreover, the endoscopists may themselves be at significant risk of contamination. Fecal-oral transmission of the infection is possible, especially insofar as viral shedding in stools seems frequent and of longer duration than at the ENT level, including in patients with negative throat swab and without digestive symptoms. In some doubtful cases, virologic assessment of stool samples can yield definitive diagnosis. In the event of prolonged viral shedding in stools, a patient's persistent contagiousness is conceivable but not conclusively established. Upcoming serology should enable identification of the patients having been infected by the COVID-19 epidemic, particularly among previously undetected pauci-symptomatic members of a health care staff. Resumption of medico-surgical activity should be the object of a dedicated strategy preceding deconfinement.
与新型冠状病毒肺炎(COVID-19)相关的症状主要表现为发热、干咳和呼吸困难三联征。然而,也有消化系统症状的报道。起初认为这些症状不常见,但实际上似乎影响了超过半数的患者。症状主要包括食欲不振、腹泻、恶心和/或呕吐以及腹痛。尽管预后与肺损伤相关,但在患有严重COVID-19感染的患者中,消化系统症状似乎更为常见。确实有消化系统表现的报道,这些表现可能是孤立的,也可能先于肺部症状出现,腹泻是主要的临床症状。早期提示COVID-19感染的主要生物学异常是淋巴细胞减少、C反应蛋白升高和天冬氨酸转氨酶升高。胸腹扫描似乎有助于一方面排除与冠状病毒无关的消化系统病变,另一方面寻找与COVID-19感染相符的肺部影像。对于持续性消化系统症状的病例,目前尚无关于消化内镜检查价值的数据。此外,内镜检查人员自身可能面临显著的污染风险。感染通过粪口传播是可能的,特别是考虑到粪便中的病毒排出似乎很常见,且持续时间比耳鼻喉部位更长,包括咽拭子阴性且无消化系统症状的患者。在一些可疑病例中,对粪便样本进行病毒学评估可得出明确诊断。如果粪便中病毒排出时间延长,可以想象患者会持续具有传染性,但尚未得到确凿证实。即将开展的血清学检测应能够识别感染过COVID-19疫情的患者,特别是在医护人员中那些之前未被发现的轻症患者。在解除隔离之前,恢复医疗外科活动应成为一项专门策略的目标。