Gagnat Yngvild, Brændvik Siri Merete, Roeleveld Karin
Clinic for Orthopaedics, Rheumatology and Skin Diseases, Orthopaedic Research Center, St. Olavs University Hospital, Trondheim, Norway.
Department of Neuromedicine and Movement Science, Faculty of Medicine and Health, Norwegian University of Science and Technology, NTNU, Trondheim, Norway.
Front Neurol. 2020 Apr 17;11:202. doi: 10.3389/fneur.2020.00202. eCollection 2020.
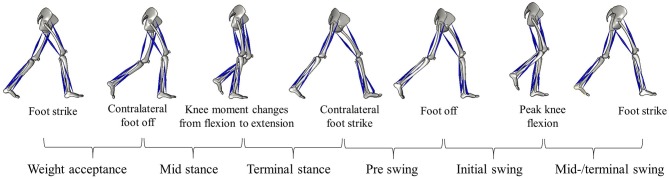
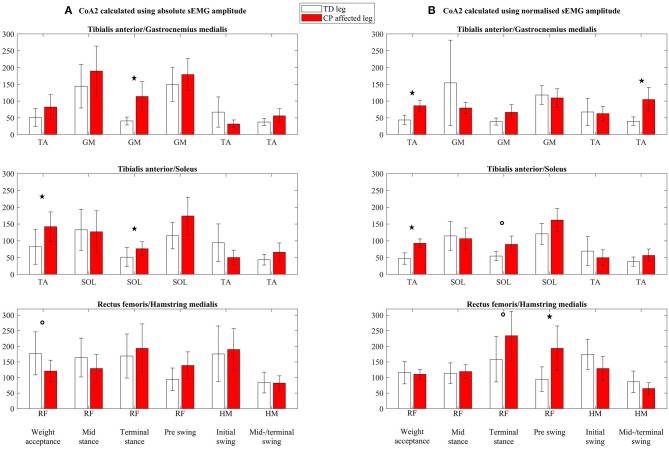
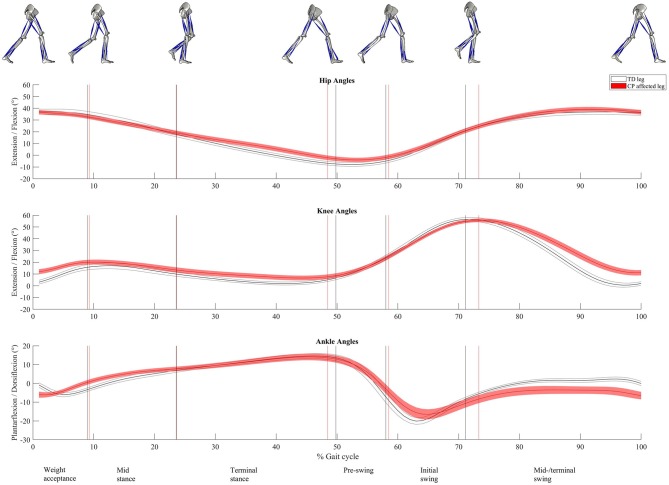
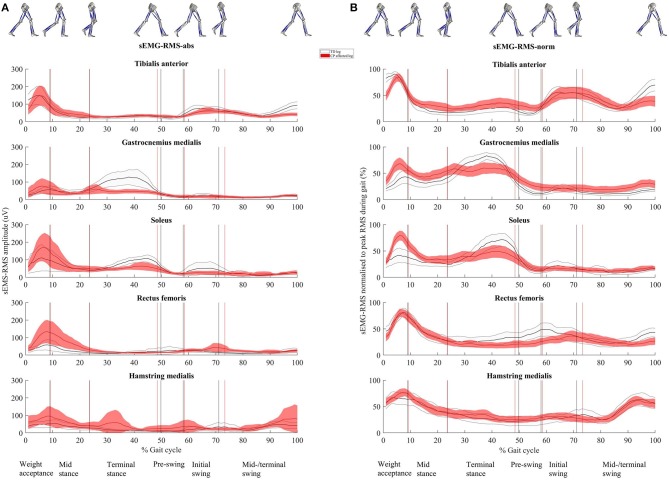
Investigating muscle activity and coactivation with surface electromyography (sEMG) gives insight into pathological muscle function during activities like walking in people with neuromuscular impairments, such as children with cerebral palsy (CP). There is large variation in the amount of coactivation reported during walking in children with CP, possibly due to the inconsistent handling of sEMG and in calculating the coactivation index. The aim of this study was to evaluate how different approaches of handling sEMG may affect the interpretation of muscle activity and coactivation, by looking at both absolute and normalized sEMG. Twenty-three ambulatory children with CP and 11 typically developing (TD) children participated. We conducted a three-dimensional gait analysis (3DGA) with concurrent sEMG measurements of tibialis anterior, soleus, gastrocnemius medialis, rectus femoris, and hamstring medialis. They walked barefoot at a self-selected, comfortable speed back and forth a 7-m walkway. The gait cycle extracted from the 3DGA was divided into six phases, and for each phase, root mean square sEMG amplitude was calculated (sEMG-RMS-abs), and also normalized to peak amplitude of the linear envelope (50-ms running RMS window) during the gait cycle (sEMG-RMS-norm). The coactivation index was calculated using sEMG-RMS-abs and sEMG-RMS-norm values and by using two different indices. Differences between TD children's legs and the affected legs of children with CP were tested with a mixed model. The between-subject muscle activity variability was more evenly distributed using sEMG-RMS-norm; however, potential physiological variability was eliminated as a result of normalization. Differences between groups in one gait phase using sEMG-RMS-abs showed opposite differences in another phase using sEMG-RMS-norm for three of the five muscles investigated. The CP group showed an increased coactivation index in two out of three muscle pairs using sEMG-RMS-abs and in all three muscle pairs using sEMG-RMS-norm. These results were independent of index calculation method. Moreover, the increased coactivation indices could be explained by either reduced agonist activity or increased antagonist activity. Thus, differences in muscle activity and coactivation index between the groups change after normalization. However, because we do not know the truth, we cannot conclude whether to normalize and recommend incorporating both.
利用表面肌电图(sEMG)研究肌肉活动和共同激活,有助于深入了解神经肌肉功能障碍患者(如脑性瘫痪(CP)儿童)在行走等活动中的病理性肌肉功能。据报道,CP儿童在行走过程中的共同激活量存在很大差异,这可能是由于对sEMG的处理以及共同激活指数计算方法不一致所致。本研究的目的是通过观察绝对和归一化的sEMG,评估不同的sEMG处理方法如何影响对肌肉活动和共同激活的解释。23名能行走的CP儿童和11名发育正常(TD)的儿童参与了研究。我们进行了三维步态分析(3DGA),同时测量胫骨前肌、比目鱼肌、腓肠肌内侧头、股直肌和半腱肌的sEMG。他们赤足以自我选择的舒适速度在7米长的通道上来回行走。从3DGA中提取的步态周期分为六个阶段,对于每个阶段,计算均方根sEMG幅度(sEMG-RMS-abs),并将其归一化为步态周期内线性包络的峰值幅度(50毫秒运行均方根窗口)(sEMG-RMS-norm)。使用sEMG-RMS-abs和sEMG-RMS-norm值以及两种不同的指数计算共同激活指数。使用混合模型测试TD儿童的双腿与CP儿童受影响腿之间的差异。使用sEMG-RMS-norm时,受试者间肌肉活动变异性分布更均匀;然而,归一化导致潜在的生理变异性被消除。在所研究的五块肌肉中的三块中,使用sEMG-RMS-abs在一个步态阶段的组间差异与使用sEMG-RMS-norm在另一个步态阶段的差异相反。CP组在使用sEMG-RMS-abs时,三对肌肉中有两对的共同激活指数增加,在使用sEMG-RMS-norm时,三对肌肉的共同激活指数均增加。这些结果与指数计算方法无关。此外,共同激活指数的增加可以通过激动剂活性降低或拮抗剂活性增加来解释。因此,归一化后两组之间的肌肉活动和共同激活指数差异会发生变化。然而,由于我们不知道真相,我们无法得出是否进行归一化的结论,并建议同时采用两种方法。