Department of Gastroenterology and Hepatology, University of Groningen, University Medical Center Groningen, Groningen, The Netherlands.
Department of Genetics, University of Groningen, University Medical Center Groningen, Groningen, The Netherlands.
Aliment Pharmacol Ther. 2020 Jun;51(11):1105-1115. doi: 10.1111/apt.15762. Epub 2020 May 3.
High inter-individual variability in therapeutic response to drugs used in the management of Inflammatory Bowel Disease (IBD) leads to high morbidity and high costs. Genetic variants predictive of thiopurine-induced myelosuppression, thiopurine-induced pancreatitis and immunogenicity of Tumour Necrosis Factor alpha (TNFα) antagonists have been identified, but uptake of pre-treatment pharmacogenetic testing into clinical guidelines has been slow.
To explore the efficacy of a pharmacogenetic passport for IBD that includes multiple pharmacogenetic predictors of response.
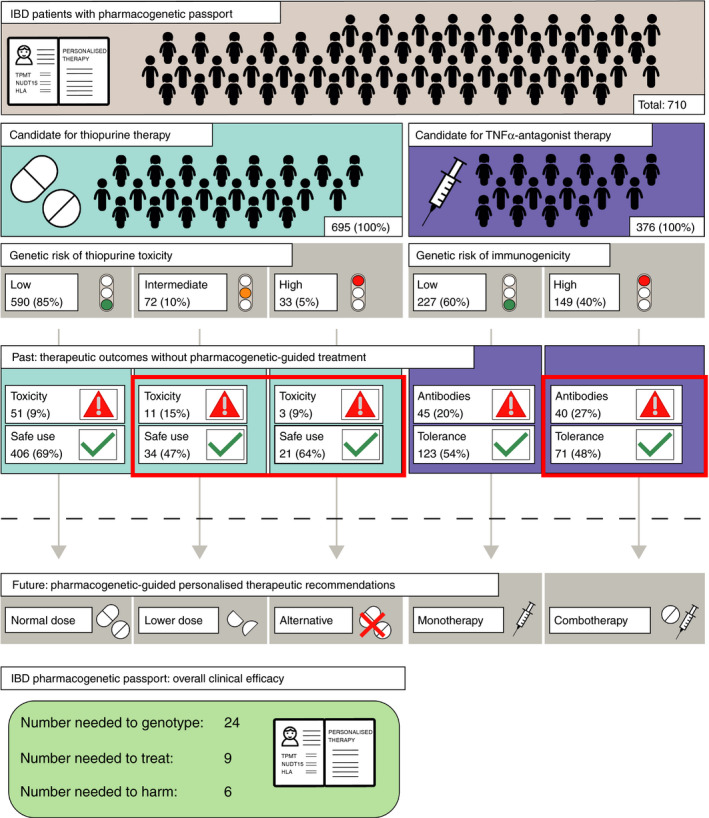
Patients with IBD exposed to thiopurines and/or TNFα antagonists were retrospectively evaluated for the presence of thiopurine toxicity and/or immunogenicity of TNFα antagonists. All patients were genotyped using both whole-exome sequencing and the Illumina Global Screening Array. An in-house-developed computational pipeline translated genetic data into an IBD pharmacogenetic passport that predicted risks for thiopurine toxicity and immunogenicity of TNFα antagonists per patient. Using pharmacogenetic-guided treatment guidelines, we calculated clinical efficacy estimates for pharmacogenetic testing for IBD.
Among 710 patients with IBD exposed to thiopurines and/or TNFα antagonists, 150 adverse drug responses occurred and our pharmacogenetic passport would have predicted 54 (36%) of these. Using a pharmacogenetic passport for IBD that includes genetic variants predictive of thiopurine-induced myelosuppression, thiopurine-induced pancreatitis, and immunogenicity of TNFα antagonists, 24 patients need to be genotyped to prevent one of these adverse drug responses.
This study highlights the clinical efficacy of a pharmacogenetic passport for IBD. Implementation of such a pharmacogenetic passport into clinical management of IBD may contribute to a reduction in adverse drug responses.
在炎症性肠病(IBD)的管理中使用的药物治疗反应存在个体间高度变异性,导致高发病率和高成本。已经确定了预测硫嘌呤诱导的骨髓抑制、硫嘌呤诱导的胰腺炎和肿瘤坏死因子α(TNFα)拮抗剂免疫原性的遗传变异,但治疗前药物遗传学检测纳入临床指南的速度较慢。
探索包含多种药物反应预测因子的 IBD 药物遗传学护照的疗效。
回顾性评估接受硫嘌呤和/或 TNFα 拮抗剂治疗的 IBD 患者是否存在硫嘌呤毒性和/或 TNFα 拮抗剂的免疫原性。所有患者均使用全外显子组测序和 Illumina 全球筛选阵列进行基因分型。我们使用内部开发的计算管道将遗传数据转化为 IBD 药物遗传学护照,预测每位患者硫嘌呤毒性和 TNFα 拮抗剂免疫原性的风险。使用药物遗传学指导的治疗指南,我们计算了 IBD 药物遗传学检测的临床疗效估计。
在 710 名接受硫嘌呤和/或 TNFα 拮抗剂治疗的 IBD 患者中,发生了 150 例药物不良反应,我们的药物遗传学护照预测了其中的 54 例(36%)。使用包含预测硫嘌呤诱导的骨髓抑制、硫嘌呤诱导的胰腺炎和 TNFα 拮抗剂免疫原性的遗传变异的 IBD 药物遗传学护照,需要对 24 名患者进行基因分型,以预防其中一种药物不良反应。
本研究强调了 IBD 药物遗传学护照的临床疗效。将这种药物遗传学护照纳入 IBD 的临床管理可能有助于减少药物不良反应。